

The gravitational distribution of ventilation-perfusion ratio is more uniform in prone than supine posture in the normal human lung
- PMID: 23620488
- PMCID: PMC3743008
- DOI: 10.1152/japplphysiol.01531.2012
The gravitational distribution of ventilation-perfusion ratio is more uniform in prone than supine posture in the normal human lung
Abstract
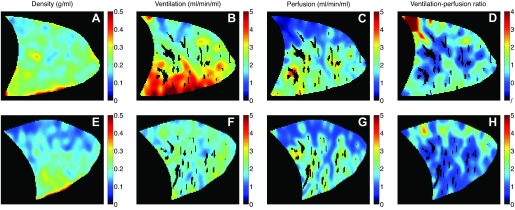
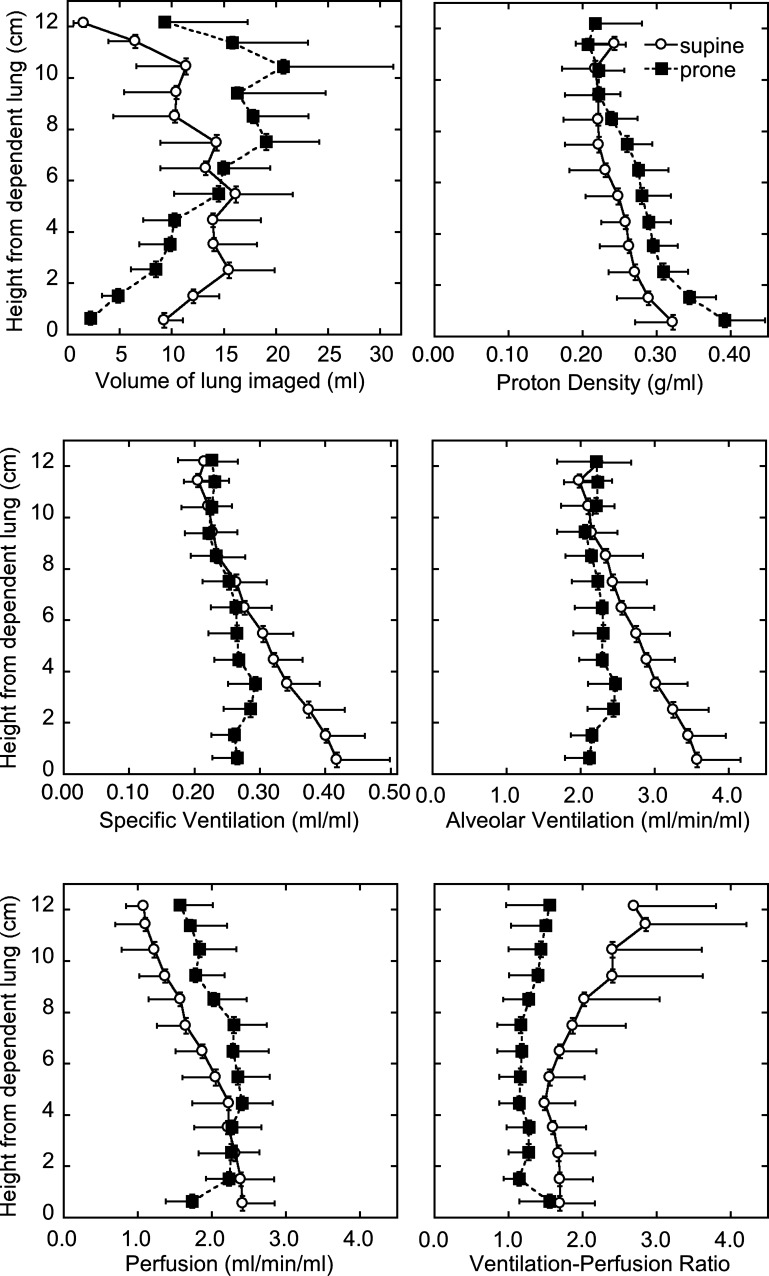
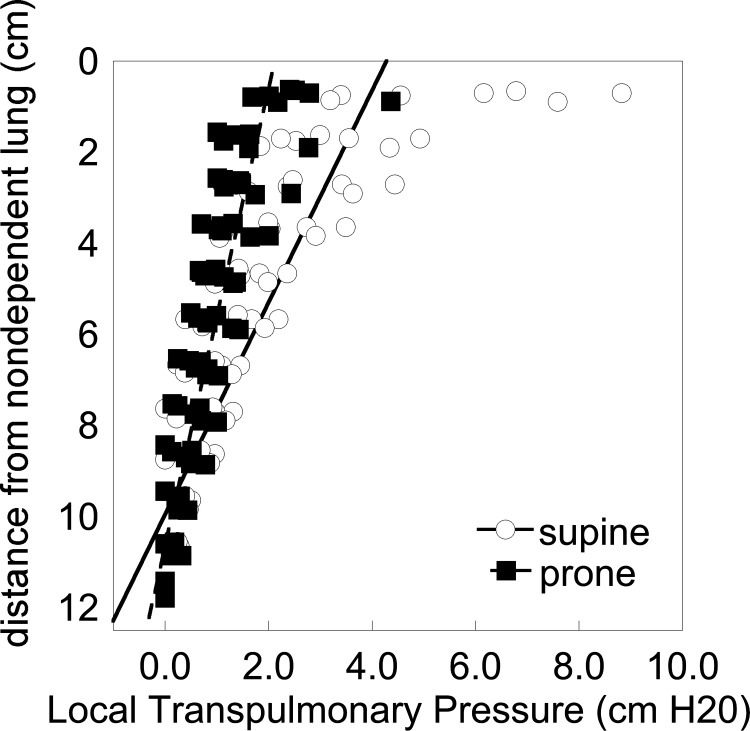
The gravitational gradient of intrapleural pressure is suggested to be less in prone posture than supine. Thus the gravitational distribution of ventilation is expected to be more uniform prone, potentially affecting regional ventilation-perfusion (Va/Q) ratio. Using a novel functional lung magnetic resonance imaging technique to measure regional Va/Q ratio, the gravitational gradients in proton density, ventilation, perfusion, and Va/Q ratio were measured in prone and supine posture. Data were acquired in seven healthy subjects in a single sagittal slice of the right lung at functional residual capacity. Regional specific ventilation images quantified using specific ventilation imaging and proton density images obtained using a fast gradient-echo sequence were registered and smoothed to calculate regional alveolar ventilation. Perfusion was measured using arterial spin labeling. Ventilation (ml·min(-1)·ml(-1)) images were combined on a voxel-by-voxel basis with smoothed perfusion (ml·min(-1)·ml(-1)) images to obtain regional Va/Q ratio. Data were averaged for voxels within 1-cm gravitational planes, starting from the most gravitationally dependent lung. The slope of the relationship between alveolar ventilation and vertical height was less prone than supine (-0.17 ± 0.10 ml·min(-1)·ml(-1)·cm(-1) supine, -0.040 ± 0.03 prone ml·min(-1)·ml(-1)·cm(-1), P = 0.02) as was the slope of the perfusion-height relationship (-0.14 ± 0.05 ml·min(-1)·ml(-1)·cm(-1) supine, -0.08 ± 0.09 prone ml·min(-1)·ml(-1)·cm(-1), P = 0.02). There was a significant gravitational gradient in Va/Q ratio in both postures (P < 0.05) that was less in prone (0.09 ± 0.08 cm(-1) supine, 0.04 ± 0.03 cm(-1) prone, P = 0.04). The gravitational gradients in ventilation, perfusion, and regional Va/Q ratio were greater supine than prone, suggesting an interplay between thoracic cavity configuration, airway and vascular tree anatomy, and the effects of gravity on Va/Q matching.
Keywords: arterial spin labeling; gravity; magnetic resonance imaging; specific ventilation imaging; ventilation-perfusion ratio.
Figures
Comment in
-
Imaging tools for the investigation of human gas exchange.J Appl Physiol (1985). 2013 Aug 1;115(3):309-10. doi: 10.1152/japplphysiol.00591.2013. Epub 2013 May 23. J Appl Physiol (1985). 2013. PMID: 23703120 No abstract available.
Similar articles
-
Interrelationships between regional blood flow, blood volume, and ventilation in supine humans.J Appl Physiol (1985). 1994 Mar;76(3):1205-10. doi: 10.1152/jappl.1994.76.3.1205. J Appl Physiol (1985). 1994. PMID: 8005864
-
Lung ventilation and perfusion in prone and supine postures with reference to anesthetized and mechanically ventilated healthy volunteers.Anesthesiology. 2010 Mar;112(3):682-7. doi: 10.1097/ALN.0b013e3181cf40c8. Anesthesiology. 2010. PMID: 20179506
-
Regional ventilation-perfusion distribution is more uniform in the prone position.J Appl Physiol (1985). 2000 Mar;88(3):1076-83. doi: 10.1152/jappl.2000.88.3.1076. J Appl Physiol (1985). 2000. PMID: 10710406
-
Pathophysiology of prone positioning in the healthy lung and in ALI/ARDS.Minerva Anestesiol. 2001 Apr;67(4):238-47. Minerva Anestesiol. 2001. PMID: 11376516 Review.
-
Therapeutic benefits of proning to improve pulmonary gas exchange in severe respiratory failure: focus on fundamentals of physiology.Exp Physiol. 2022 Jul;107(7):759-770. doi: 10.1113/EP089405. Epub 2021 Aug 13. Exp Physiol. 2022. PMID: 34242438 Free PMC article. Review.
Cited by
-
Awake Proning: A Necessary Evil During the COVID-19 Pandemic.Cureus. 2020 Jul 3;12(7):e8989. doi: 10.7759/cureus.8989. Cureus. 2020. PMID: 32775071 Free PMC article. Review.
-
Recruitment Maneuvers and Higher PEEP, the So-Called Open Lung Concept, in Patients with ARDS.Crit Care. 2019 Mar 9;23(1):73. doi: 10.1186/s13054-019-2365-1. Crit Care. 2019. PMID: 30850004 Free PMC article. Review.
-
A framework for heart-lung interaction and its application to prone position in the acute respiratory distress syndrome.Front Physiol. 2023 Aug 7;14:1230654. doi: 10.3389/fphys.2023.1230654. eCollection 2023. Front Physiol. 2023. PMID: 37614757 Free PMC article.
-
Validating the distribution of specific ventilation in healthy humans measured using proton MR imaging.J Appl Physiol (1985). 2014 Apr 15;116(8):1048-56. doi: 10.1152/japplphysiol.00982.2013. Epub 2014 Feb 6. J Appl Physiol (1985). 2014. PMID: 24505099 Free PMC article.
-
Quantitative Computed Tomography and Response to Pronation in COVID-19 ARDS.Respir Care. 2024 Oct 25;69(11):1380-1391. doi: 10.4187/respcare.11625. Respir Care. 2024. PMID: 38594036
References
-
- Albert RK, Hubmayr RD. The prone position eliminates compression of the lungs by the heart. Am J Respir Crit Care Med 161: 1660–1665, 2000 - PubMed
-
- Amis TC, Jones HA, Hughes JM. Effect of posture on inter-regional distribution of pulmonary perfusion and V̇a/Q̇ ratios in man. Respir Physiol 56: 169–182, 1984 - PubMed
-
- Arnold JF, Fidler F, Wang T, Pracht ED, Schmidt M, Jakob PM. Imaging lung function using rapid dynamic acquisition of T1-maps during oxygen enhancement. MAGMA 16: 246–253, 2004 - PubMed
-
- Bolar DS, Levin DL, Hopkins SR, Frank LF, Liu TT, Wong EC, Buxton RB. Quantification of regional pulmonary blood flow using ASL-FAIRER. Magn Reson Med 55: 1308–1317, 2006 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous