

Bone- and dentoalveolar-anchored dentofacial orthopedics for Class III malocclusion: new approaches, similar objectives? : a systematic review
- PMID: 23621558
- PMCID: PMC8763068
- DOI: 10.2319/051312-392.1
Bone- and dentoalveolar-anchored dentofacial orthopedics for Class III malocclusion: new approaches, similar objectives? : a systematic review
Abstract
Objectives: To analyze the scientific literature and compare in the results of conventional orthopedic appliances with those obtained from recent bone-anchored orthopedics for Class III malocclusion.
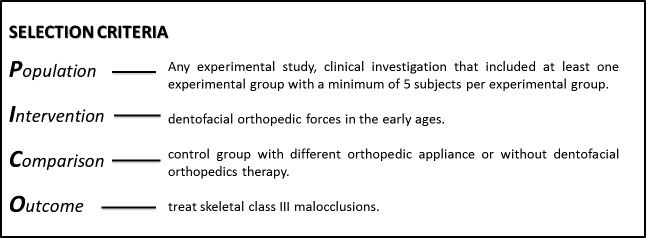
Materials and methods: The literature was systematically reviewed using PubMed/Medline, Scopus, and Scirus databases up to January 2012. Articles were selected by two different researchers (kappa index = 0.83), based on established inclusion/exclusion criteria. Methodologic quality was classified as high, medium, or low quality.
Results: The search strategy identified 1020 titles. Thirty studies were selected after applying the criteria (high quality = 9, medium quality = 21). Protraction rates differed within a range of one- to twofold between bone-anchored and dentoalveolar therapies (P < .001). All studies noted the effect of clockwise rotation on the mandible and an increase in inferior-anterior and total facial height; this was more obvious in dentoalveolar therapy than in bone-anchored orthopedics (P < .001).
Conclusions: Dental parameters like overjet increased significantly with both sets of groups, ranging from 1.7 to 7.9 mm with dentoalveolar therapy and from 2.7 to 7.6 mm with bone-anchored orthopedics.
Figures
References
-
- Keles A, Tokmak EC, Erverdi N, Nanda R. Effect of varying the force direction on maxillary orthopedic protraction. Angle Orthod. 2002;72:387–396. - PubMed
-
- Toffol LD, Pavoni C, Baccetti T, Franchi L, Cozza P. Orthopedic treatment outcomes in Class III malocclusion. Angle Orthod. 2008;78:561–573. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
