

The effects of the semirecumbent position on hemodynamic status in patients on invasive mechanical ventilation: prospective randomized multivariable analysis
- PMID: 23622019
- PMCID: PMC4056784
- DOI: 10.1186/cc12694
The effects of the semirecumbent position on hemodynamic status in patients on invasive mechanical ventilation: prospective randomized multivariable analysis
Abstract
Introduction: Adopting the 45° semirecumbent position in mechanically ventilated critically ill patients is recommended, as it has been shown to reduce the incidence of ventilator-associated pneumonia. Although the benefits to the respiratory system are clear, it is not known whether elevating the head of the bed results in hemodynamic instability. We examined the effect of head of bed elevation (HBE) on hemodynamic status and investigated the factors that influence mean arterial pressure (MAP) and central venous oxygen saturation (ScvO2) when patients were positioned at 0°, 30°, and 45°.
Methods: Two hundred hemodynamically stable adults on invasive mechanical ventilation admitted to a multidisciplinary surgical intensive care unit were recruited. Patients' characteristics included catecholamine and sedative doses, the original angle of head of bed elevation (HBE), the level of positive end expiratory pressure (PEEP), duration and mode of mechanical ventilation. A sequence of HBE positions (0°, 30°, and 45°) was adopted in random order, and MAP and ScvO2 were measured at each position. Patients acted as their own controls. The influence of degree of HBE and of the covariables on MAP and ScvO2 was analyzed by using liner mixed models. Additionally, uni- and multivariable logistic regression models were used to indentify risk factors for hypotension during HBE, defined as MAP <65 mmHg.
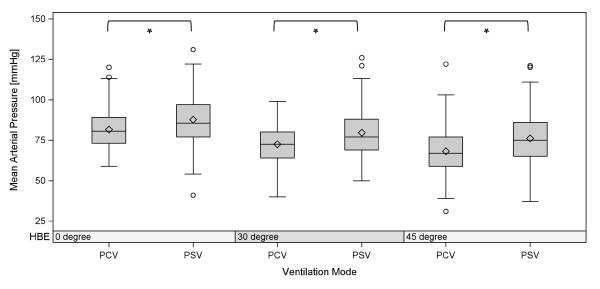
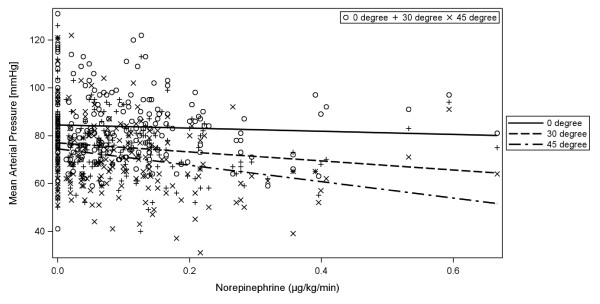
Results: Changing HBE from supine to 45° caused significant reductions in MAP (from 83.8 mmHg to 71.1 mmHg, P < 0.001) and ScvO2 (76.1% to 74.3%, P < 0.001). Multivariable modeling revealed that mode and duration of mechanical ventilation, the norepinephrine dose, and HBE had statistically significant influences. Pressure-controlled ventilation was the most influential risk factor for hypotension when HBE was 45° (odds ratio (OR) 2.33, 95% confidence interval (CI), 1.23 to 4.76, P = 0.017).
Conclusions: HBE to the 45° position is associated with significant decreases in MAP and ScvO2 in mechanically ventilated patients. Pressure-controlled ventilation, higher simplified acute physiology (SAPS II) score, sedation, high catecholamine, and PEEP requirements were identified as independent risk factors for hypotension after backrest elevation. Patients at risk may need positioning at 20° to 30° to overcome the negative effects of HBE, especially in the early phase of intensive care unit admission.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
