

Targeted rotavirus vaccination of high-risk infants; a low cost and highly cost-effective alternative to universal vaccination
- PMID: 23622110
- PMCID: PMC3665442
- DOI: 10.1186/1741-7015-11-112
Targeted rotavirus vaccination of high-risk infants; a low cost and highly cost-effective alternative to universal vaccination
Abstract
Background: The cost-effectiveness of universal rotavirus (RV) vaccination is controversial in developed countries. As a result, RV vaccination programs do not currently exist in most European countries. Hospitalization is the main driver of RV disease costs, and prematurity, low birth weight (LBW) and underlying medical conditions have been associated with RV hospitalization and complications. We investigated the cost-effectiveness of targeted RV vaccination of high-risk infants and universal RV vaccination versus no vaccination.
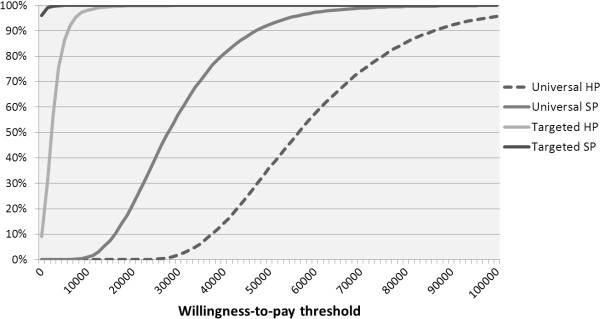
Methods: Disease burden, mortality and healthcare costs of RV hospitalization for children with and without prematurity, LBW and congenital pathology were quantified in two hospital-based observational studies in the Netherlands. Cost-effectiveness analysis was based on an age-structured stochastic multi-cohort model of the Dutch population comparing universal RV vaccination and targeted vaccination of high-risk infants to no vaccination. The primary endpoint was the incremental cost-effectiveness ratio (ICER), with a threshold of €35,000/quality-adjusted life year (QALY) from the healthcare provider perspective. Sensitivity analyses included vaccine price and coverage, herd-immunity and QALY losses.
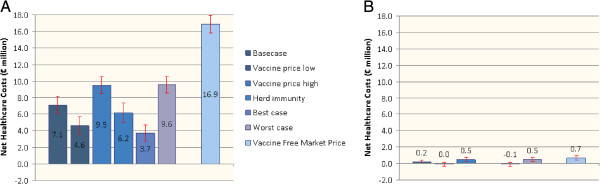
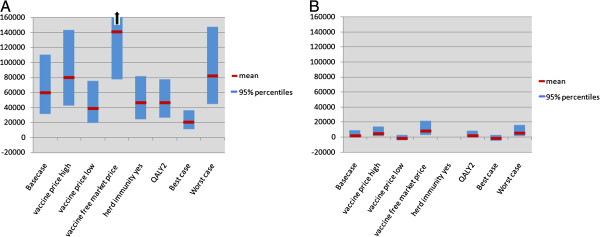
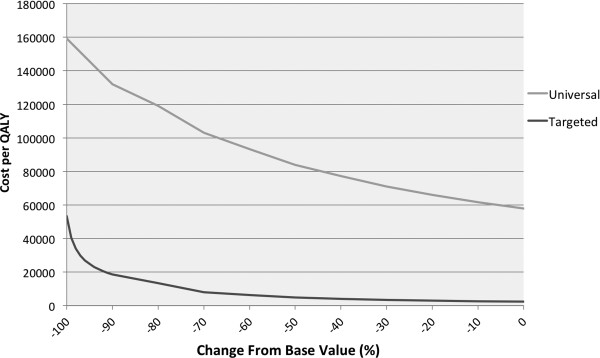
Results: A total of 936 children with RV infection were included. Prematurity, LBW and congenital pathology were associated with increased risks of RV hospitalization (relative risks (RR) ranging from 1.6 to 4.4), ICU admission (RR ranging from 4.2 to 7.9), prolonged hospital stay (1.5 to 3.0 excess days) and higher healthcare costs (€648 to €1,533 excess costs). Seven children succumbed due to RV complications, all belonging to the high-risk population. Targeted RV vaccination was highly cost-effective and potentially cost-saving from the healthcare provider perspective with ICERs below €20,000/QALY in all scenarios with total (undiscounted) annual healthcare costs between -€0.1 and €0.5 million/year. Results were most sensitive to mortality rates, but targeted vaccination remained highly cost-effective up to reductions of 90% compared to observed mortality. Universal RV vaccination was not considered cost-effective (mean ICER: €60,200/QALY) unless herd-immunity and caretaker QALY losses were included and vaccine prices were €60 at most (mean ICER: €21,309/QALY).
Conclusion: We recommend targeted RV vaccination for high-risk infants in developed countries.
Figures
Similar articles
-
Updated cost-effectiveness and risk-benefit analysis of two infant rotavirus vaccination strategies in a high-income, low-endemic setting.BMC Med. 2018 Sep 10;16(1):168. doi: 10.1186/s12916-018-1134-3. BMC Med. 2018. PMID: 30196794 Free PMC article.
-
Cost-effectiveness of universal rotavirus vaccination in reducing rotavirus gastroenteritis in Ireland.Vaccine. 2011 Oct 6;29(43):7463-73. doi: 10.1016/j.vaccine.2011.07.056. Epub 2011 Aug 5. Vaccine. 2011. PMID: 21821085
-
Cost-effectiveness of childhood rotavirus vaccination in Germany.Vaccine. 2014 Apr 7;32(17):1964-74. doi: 10.1016/j.vaccine.2014.01.061. Epub 2014 Feb 20. Vaccine. 2014. PMID: 24561052
-
Rotavirus vaccine RIX4414 (Rotarix™): a pharmacoeconomic review of its use in the prevention of rotavirus gastroenteritis in developed countries.Pharmacoeconomics. 2011 May;29(5):439-54. doi: 10.2165/11207130-000000000-00000. Pharmacoeconomics. 2011. PMID: 21504245 Review.
-
A critical literature review of health economic evaluations of rotavirus vaccination.Hum Vaccin Immunother. 2013 Jun;9(6):1272-88. doi: 10.4161/hv.24253. Epub 2013 Apr 9. Hum Vaccin Immunother. 2013. PMID: 23571226 Free PMC article. Review.
Cited by
-
Rotavirus Vaccination of Infants Delayed and Limited within the National Immunization Programme in the Netherlands: An Opportunity Lost.Vaccines (Basel). 2021 Feb 10;9(2):144. doi: 10.3390/vaccines9020144. Vaccines (Basel). 2021. PMID: 33579025 Free PMC article.
-
Potential safety issues and other factors that may affect the introduction and uptake of rotavirus vaccines.Clin Microbiol Infect. 2016 Dec 1;22 Suppl 5(Suppl 5):S128-S135. doi: 10.1016/j.cmi.2016.03.007. Epub 2016 Apr 26. Clin Microbiol Infect. 2016. PMID: 27129416 Free PMC article.
-
Economics and financing of vaccines for diarrheal diseases.Hum Vaccin Immunother. 2014;10(6):1568-81. doi: 10.4161/hv.28885. Epub 2014 Apr 22. Hum Vaccin Immunother. 2014. PMID: 24755623 Free PMC article. Review.
-
Updated cost-effectiveness and risk-benefit analysis of two infant rotavirus vaccination strategies in a high-income, low-endemic setting.BMC Med. 2018 Sep 10;16(1):168. doi: 10.1186/s12916-018-1134-3. BMC Med. 2018. PMID: 30196794 Free PMC article.
-
Pediatric complex chronic conditions classification system version 2: updated for ICD-10 and complex medical technology dependence and transplantation.BMC Pediatr. 2014 Aug 8;14:199. doi: 10.1186/1471-2431-14-199. BMC Pediatr. 2014. PMID: 25102958 Free PMC article.
References
-
- Committee on Infectious Diseases. Prevention of rotavirus disease: updated guidelines for use of rotavirus vaccine. Pediatrics. 2009;123:1412–1420. - PubMed
-
- Cortese MM, Parashar UD. Prevention of rotavirus gastroenteritis among infants and children: recommendations of the Advisory Committee on Immunization Practices (ACIP) MMWR Recomm Rep. 2009;58:1–25. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
