

Characteristics of children and young adults with Marfan syndrome and aortic root dilation in a randomized trial comparing atenolol and losartan therapy
- PMID: 23622922
- PMCID: PMC4131445
- DOI: 10.1016/j.ahj.2013.02.019
Characteristics of children and young adults with Marfan syndrome and aortic root dilation in a randomized trial comparing atenolol and losartan therapy
Abstract
Background: The Pediatric Heart Network designed a clinical trial to compare aortic root growth and other short-term cardiovascular outcomes in children and young adults with Marfan syndrome randomized to receive atenolol or losartan. We report here the characteristics of the screened population and enrolled subjects.
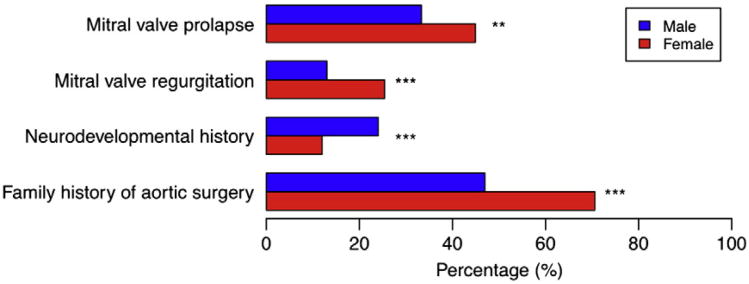
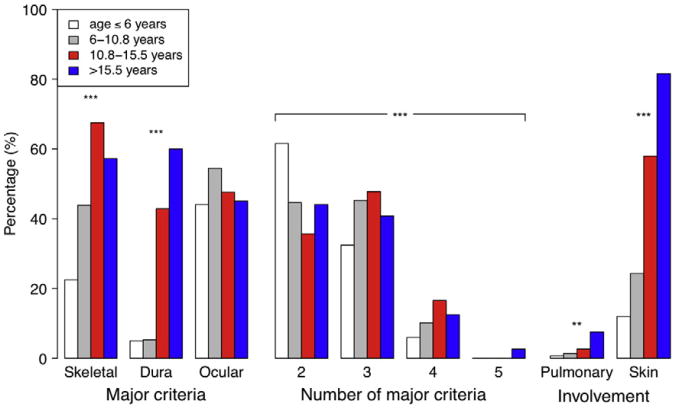
Methods and results: Between 2007 and 2011, 21 clinical sites randomized 608 subjects, aged 6 months to 25 years who met the original Ghent criteria and had a body surface area-adjusted aortic root diameter z-score >3.0. The mean age at study entry was 11.2 years, 60% were male, and 25% were older teenagers and young adults. The median aortic root diameter z-score was 4.0. Aortic root diameter z-score did not vary with age. Mitral valve prolapse and mitral regurgitation were more common in females. Among those with a positive family history, 56% had a family member with aortic surgery, and 32% had a family member with a history of aortic dissection.
Conclusions: Baseline demographic, clinical, and anthropometric characteristics of the randomized cohort are representative of patients in this population with moderate to severe aortic root dilation. The high percentage of young subjects with relatives who have had aortic dissection or surgery illustrates the need for more definitive therapy; we expect that the results of the study and the wealth of systematic data collected will make an important contribution to the management of individuals with Marfan syndrome.
Trial registration: ClinicalTrials.gov NCT00429364.
Copyright © 2013 Mosby, Inc. All rights reserved.
Figures


References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- U10 HL109741/HL/NHLBI NIH HHS/United States
- U01 HL068279/HL/NHLBI NIH HHS/United States
- U01 HL068290/HL/NHLBI NIH HHS/United States
- U01 HL068288/HL/NHLBI NIH HHS/United States
- U10 HL068270/HL/NHLBI NIH HHS/United States
- U01 HL068281/HL/NHLBI NIH HHS/United States
- U01 HL068270/HL/NHLBI NIH HHS/United States
- UL1 TR000077/TR/NCATS NIH HHS/United States
- U01 HL068292/HL/NHLBI NIH HHS/United States
- U01 HL085057/HL/NHLBI NIH HHS/United States
- U01 HL068285/HL/NHLBI NIH HHS/United States
- U01 HL068269/HL/NHLBI NIH HHS/United States
- U10 HL109816/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
