

Comparison of transcatheter and surgical aortic valve replacement in severe aortic stenosis: a longitudinal study of echocardiography parameters in cohort A of the PARTNER trial (placement of aortic transcatheter valves)
- PMID: 23623915
- PMCID: PMC3931006
- DOI: 10.1016/j.jacc.2013.02.087
Comparison of transcatheter and surgical aortic valve replacement in severe aortic stenosis: a longitudinal study of echocardiography parameters in cohort A of the PARTNER trial (placement of aortic transcatheter valves)
Abstract
Objectives: This study sought to compare echocardiographic findings in patients with critical aortic stenosis following surgical aortic valve replacement (SAVR) or transcatheter aortic valve replacement (TAVR).
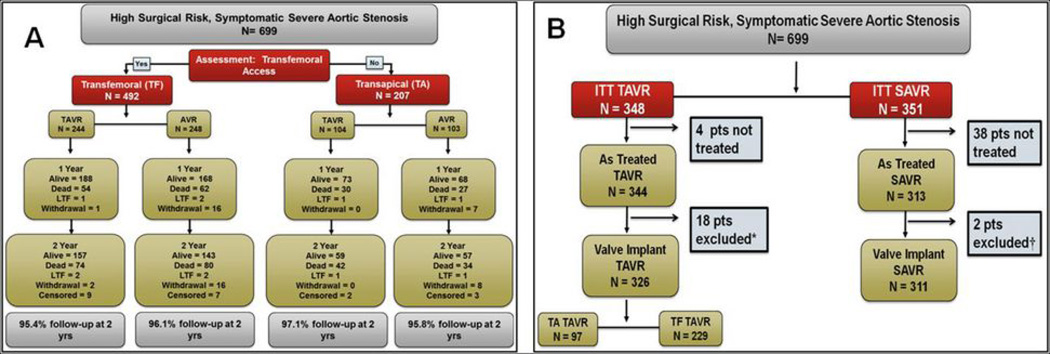
Background: The PARTNER (Placement of Aortic Transcatheter Valves) trial randomized patients 1:1 to SAVR or TAVR.
Methods: Echocardiograms were obtained at baseline, discharge, 30 days, 6 months, 1 year, and 2 years after the procedure and analyzed in a core laboratory. For the analysis of post-implantation variables, the first interpretable study (≤6 months) was used.
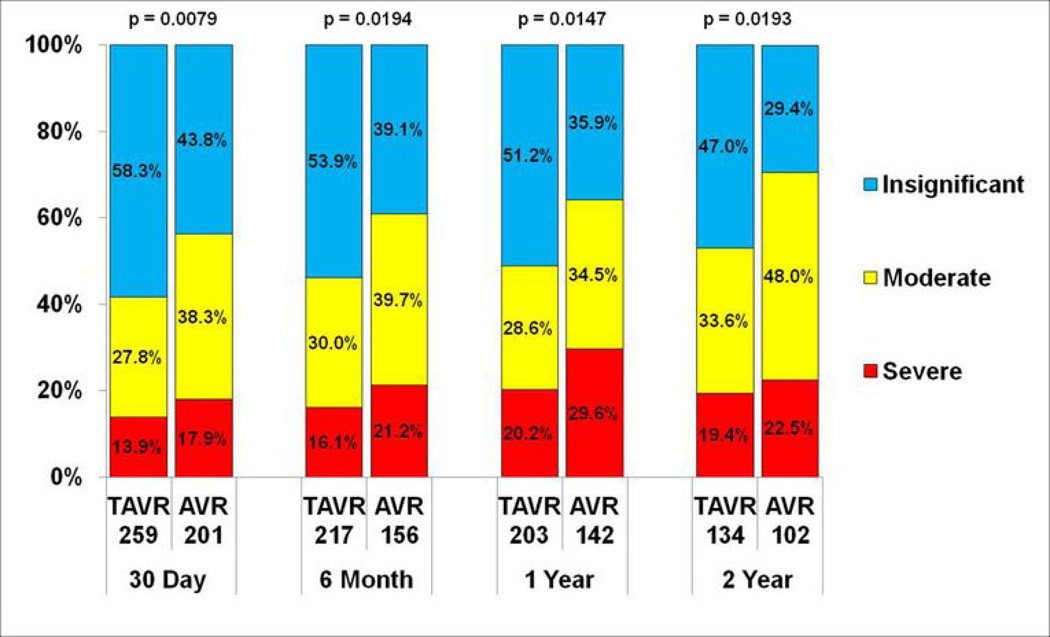
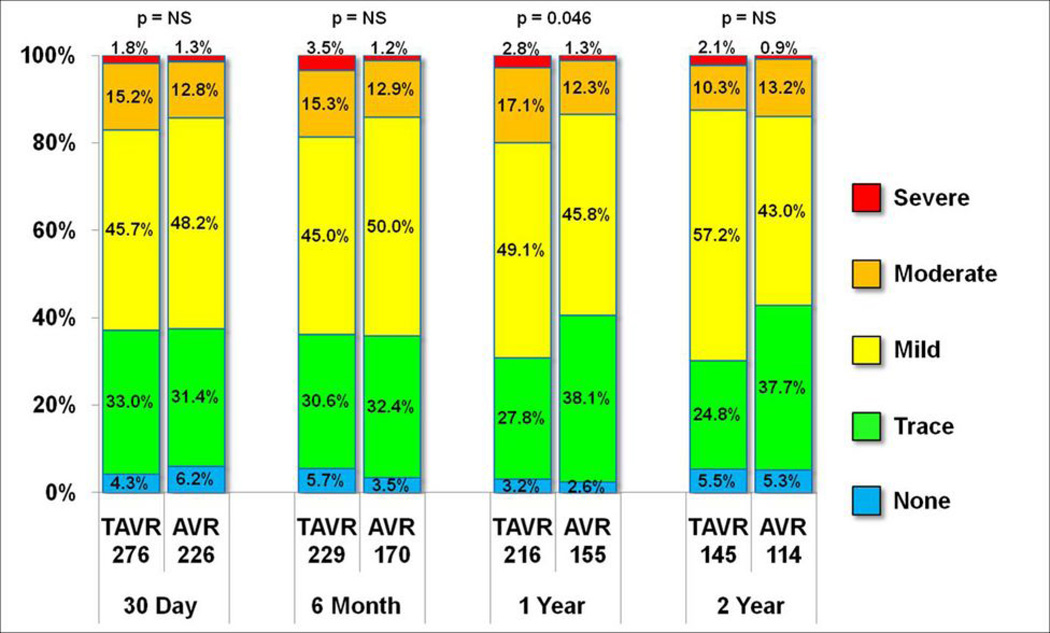
Results: Both groups showed a decrease in aortic valve gradients and increase in effective orifice area (EOA) (p < 0.0001), which remained stable over 2 years. Compared with SAVR, TAVR resulted in larger indexed EOA (p = 0.038), less prosthesis-patient mismatch (p = 0.019), and more total and paravalvular aortic regurgitation (p < 0.0001). Baseline echocardiographic univariate predictors of death were lower peak transaortic gradient in TAVR patients, and low left ventricular diastolic volume, low stroke volume, and greater severity of mitral regurgitation in SAVR patients. Post-implantation echocardiographic univariate predictors of death were: larger left ventricular diastolic volume, left ventricular systolic volume and EOA, decreased ejection fraction, and greater aortic regurgitation in TAVR patients; and smaller left ventricular systolic and diastolic volumes, low stroke volume, smaller EOA, and prosthesis-patient mismatch in SAVR patients.
Conclusions: Patients randomized to either SAVR or TAVR experience enduring, significant reductions in transaortic gradients and increase in EOA. Compared with SAVR, TAVR patients had higher indexed EOA, lower prosthesis-patient mismatch, and more aortic regurgitation. Univariate predictors of death for the TAVR and SAVR groups differed and might allow future refinement in patient selection. (THE PARTNER TRIAL: Placement of AoRTic TraNscathetER Valve Trial; NCT00530894).
Copyright © 2013 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
The other authors report no financial conflicts of interest.
Figures

Comment in
-
Evaluating the results of transcatheter versus surgical aortic valve replacement: the value of a core echocardiographic laboratory.J Am Coll Cardiol. 2013 Jun 25;61(25):2522-4. doi: 10.1016/j.jacc.2013.04.008. Epub 2013 Apr 23. J Am Coll Cardiol. 2013. PMID: 23623912 No abstract available.
References
-
- Leon MB, Smith CR, Mack M, et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med. 2010;363:1597–1607. - PubMed
-
- Smith CR, Leon MB, Mack MJ, et al. Transcatheter versus Surgical Aortic-Valve Replacement in High-Risk Patients. N Engl J Med. 2011;364:2187–2198. - PubMed
-
- Makkar RR, Fontana GP, Jilaihawi H, et al. Transcatheter Aortic-Valve Replacement for Inoperable Severe Aortic Stenosis. N Engl J Med. 2012 - PubMed
-
- Kodali SK, Williams MR, Smith CR, et al. Two-Year Outcomes after Transcatheter or Surgical Aortic-Valve Replacement. N Engl J Med. 2012 - PubMed
-
- Kodali SK, Williams MR, Smith CR, et al. Two-year outcomes after transcatheter or surgical aortic-valve replacement. The New England journal of medicine. 2012;366:1686–1695. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
