

doi: 10.4103/0974-2069.107234.
Pacing in children
Affiliations
- PMID: 23626436
- PMCID: PMC3634247
- DOI: 10.4103/0974-2069.107234
Item in Clipboard
Pacing in children
Ann Pediatr Cardiol.
2013 Jan.
Abstract
The implantation of cardiac pacing devices in children and young adults can be challenging and different from the adult population due to their smaller size, their longer life expectancy, and anatomical variations associated with congenital heart defects. A knowledge of indications, pacing leads and devices, anatomical variations, and the technical skills are important for those who implant and care for children with pacemakers. In this review we attempt to discuss these specific points of cardiac pacing in children and young adults.
Keywords: Congenital heart defects; heart block; pacemakers; pacing.
Conflict of interest statement
Figures
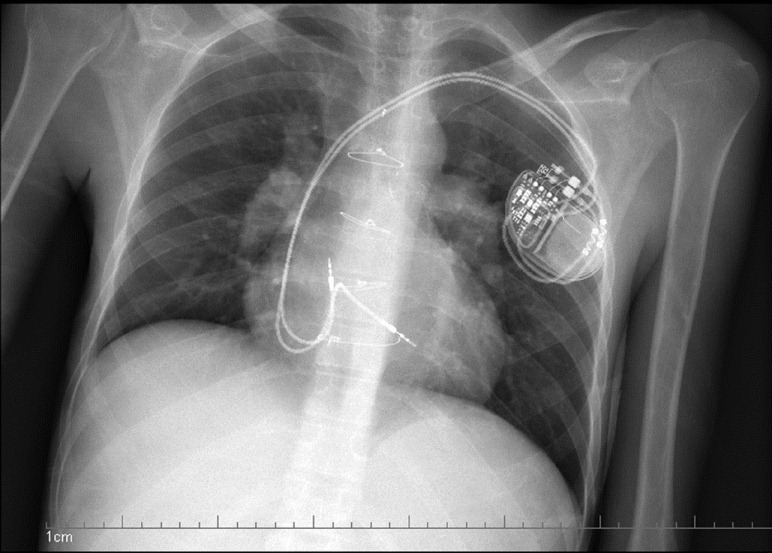
Dual chamber pacemaker showing implantation of the atrial lead in the high right atrium and septal implantation of the ventricular lead, with extra slack in the atrial and ventricular leads

The axillary venogram shows the course of the vein as it courses the junction of the outer border of the first rib with the inferior margin of the clavicle
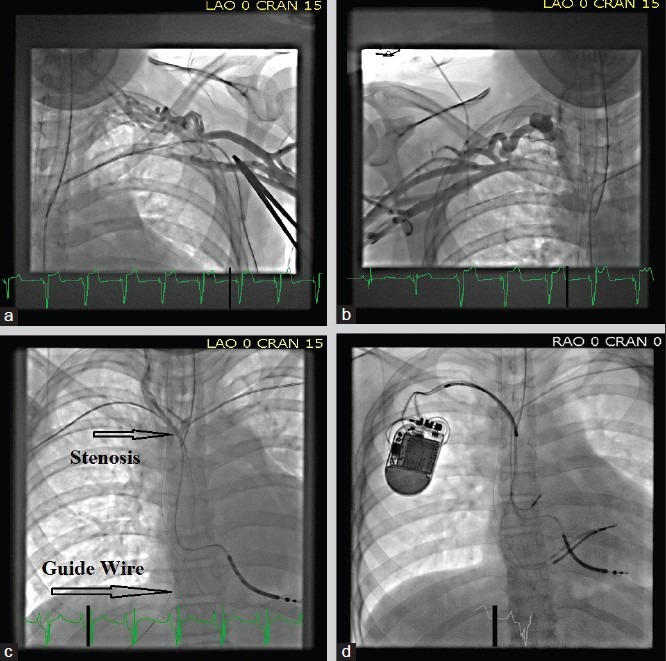
Venograms showing complete occlusion of the left subclavian (a) and proximal right subclavian (b) vein in a patient with an existing ICD lead that was fractured. (c) A guide wire (platinum plus 018, Boston scientific) was threaded from the right subclavian vein into the IVC through the stenotic site. (d) A dilator and sheath were then cannulated over the guide wire and used to pass two additional leads across this stenotic site
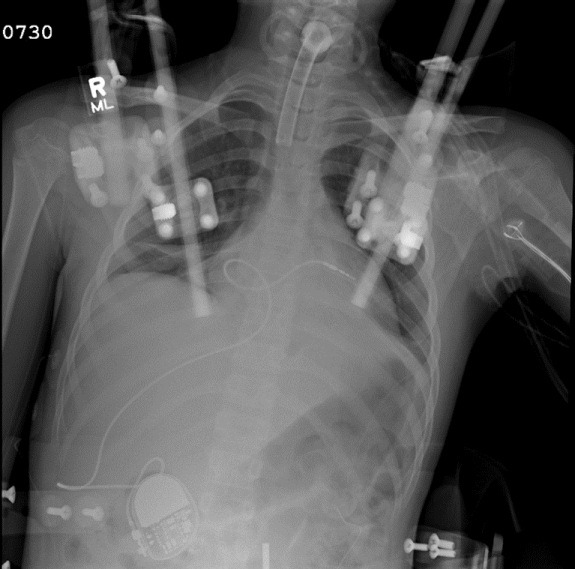
The RV lead is placed via a transhepatic approach in a 12-year-old girl for symptomatic recurrent asystolic pauses following a motor vehicular accident. She had multiple fractures of her vertebral column requiring placement of a cranial halo with traction. The access to the usual veins was limited, and therefore the lead was placed via transhepatic approach
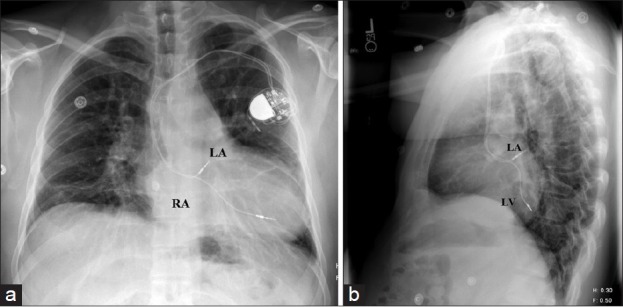
An AP and lateral view of a CXR showing a dual chamber pacemaker in a patient with Mustard procedure for D-TGA. Notice the placement of the atrial lead in the superior aspect of the left atrium and the ventricular lead in the posterior left ventricle
Similar articles
-
Cardiac pacing and defibrillation in children and young adults.Indian Pacing Electrophysiol J. 2013 Jan;13(1):4-13. doi: 10.1016/s0972-6292(16)30584-8. Epub 2013 Jan 1. Indian Pacing Electrophysiol J. 2013. PMID: 23329870 Free PMC article.
-
Efficacy of prophylactic epicardial pacing leads in children and young adults.Ann Thorac Surg. 2004 Jul;78(1):197-202; discussion 202-3. doi: 10.1016/j.athoracsur.2004.02.008. Ann Thorac Surg. 2004. PMID: 15223427 Review.
-
Pacing device therapy in infants and children: a review.J Artif Organs. 2013 Mar;16(1):23-33. doi: 10.1007/s10047-012-0668-y. Epub 2012 Oct 27. J Artif Organs. 2013. PMID: 23104398 Review.
-
Role of cardiac pacing in congenital complete heart block.Expert Rev Cardiovasc Ther. 2017 Nov;15(11):853-861. doi: 10.1080/14779072.2017.1376655. Epub 2017 Sep 13. Expert Rev Cardiovasc Ther. 2017. PMID: 28875729 Review.
-
Cardiac pacing in infants and children.Cardiol Rev. 2000 Jul-Aug;8(4):223-39. doi: 10.1097/00045415-200008040-00008. Cardiol Rev. 2000. PMID: 11174899 Review.
Cited by
-
Next-generation pacemakers: from small devices to biological pacemakers.Nat Rev Cardiol. 2018 Mar;15(3):139-150. doi: 10.1038/nrcardio.2017.165. Epub 2017 Nov 16. Nat Rev Cardiol. 2018. PMID: 29143810 Free PMC article. Review.
-
Video-assisted thoracoscopic pacemaker lead placement in children with atrioventricular block.Ann Pediatr Cardiol. 2021 Jan-Mar;14(1):67-71. doi: 10.4103/apc.APC_93_20. Epub 2020 Nov 19. Ann Pediatr Cardiol. 2021. PMID: 33679063 Free PMC article.
-
A minimally invasive approach for atrial and ventricular sew-on epicardial lead placement.JTCVS Tech. 2021 Mar 1;7:245-248. doi: 10.1016/j.xjtc.2021.02.025. eCollection 2021 Jun. JTCVS Tech. 2021. PMID: 34318263 Free PMC article. No abstract available.
-
Long-term outcome of permanent epicardial pacemaker implantation in neonates: Experience from an Indian center.Ann Pediatr Cardiol. 2024 Mar-Apr;17(2):97-100. doi: 10.4103/apc.apc_37_24. Epub 2024 Jul 20. Ann Pediatr Cardiol. 2024. PMID: 39184110 Free PMC article.
-
Intraoperative localization of cardiac conduction tissue regions using real-time fibre-optic confocal microscopy: first in human trial.Eur J Cardiothorac Surg. 2020 Aug 1;58(2):261-268. doi: 10.1093/ejcts/ezaa040. Eur J Cardiothorac Surg. 2020. PMID: 32083653 Free PMC article.
References
-
- Epstein AE, DiMarco JP, Ellenbogen KA, Estes NA, 3rd, Freedman RA, Gettes LS, et al. ACC/AHA/HRS 2008 guidelines for device-based therapy of cardiac rhythm abnormalities: A report of the american college of cardiology/American Heart Association Task Force On Practice Guidelines (Writing Committee To Revise The ACC/AHA/NASPE 2002 Guideline Update for Implantation of Cardiac Pacemakers And Antiarrhythmia Devices) Developed in Collaboration With The American Association for Thoracic Surgery and Society of Thoracic Surgeons. J Am Coll Cardiol. 2008;51:E1–62. - PubMed
-
- Cohen MI, Bush DM, Vetter VL, Tanel RE, Wieand TS, Gaynor JW, et al. Permanent epicardial pacing in pediatric patients: Seventeen years of experience and 1200 outpatient visits. Circulation. 2001;103:2585–90. - PubMed
-
- Fortescue EB, Berul CI, Cecchin F, Walsh EP, Triedman JK, Alexander ME. Patient, procedural, and hardware factors associated with pacemaker lead failures in pediatrics and Congenital Heart Disease. Heart Rhythm. 2004;1:150–9. - PubMed
-
- Sachweh JS, Vazquez-Jimenez JF, Schondube FA, Daebritz SH, Dorge H, Muhler EG, et al. Twenty years experience with pediatric pacing: Epicardial and transvenous stimulation. Eur J Cardiothorac Surg. 2000;17:455–61. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
