

doi: 10.4103/0974-2069.107235.
Pathology of Takayasu arteritis: A brief review
Affiliations
- PMID: 23626437
- PMCID: PMC3634248
- DOI: 10.4103/0974-2069.107235
Item in Clipboard
Pathology of Takayasu arteritis: A brief review
Ann Pediatr Cardiol.
2013 Jan.
Abstract
Takayasu arteritis (TA) is a chronic idiopathic and granulomatous vasculitis, manifesting mainly as a panaortitis. Autoimmune cell-mediated immunity is probably responsible for the disease. The inflammation commences from the adventitia and progresses to the intima and leads to, both in adults and children, segmental stenosis, occlusion, dilatation, and/or aneurysm formation. This review focuses briefly on the etiopathogenesis, and describes the pathological and clinical features in adults and children.
Keywords: Large vessel vasculiti; Takayasu arteritis; hypertension.
Conflict of interest statement
Figures

(a) Active phase of TA in descending thoracic aorta showing a granulomatous inflammation at the medio-adventitial junction of aorta destroying the structure of an intercostal artery; (b) chronic phase of TA in descending thoracic aorta showing media (M) at the outer third with clusters of mononuclear cells. Note marked fibrosis of the adventitia (A) (Hematoxylin and Eosin, ×250). (c) The cells are lymphocytes, and few plasma cells and histiocytes (Hematoxylin and Eosin, ×250)

Healed phase of TA in descending thoracic aorta: (a) Loose fibrocellular thickening of the intima (I); (b) junctional area between intima (I) and media (M) showing destruction of the elastic lamellae/smooth muscle with replacement fibrosis; (c) similar features are also seen toward the outer third of the media (M) and adventitia (A); (d) fibrotic adventitia (A) showing endarteritis obliterans of a branch (elastic van Gieson, ×250)

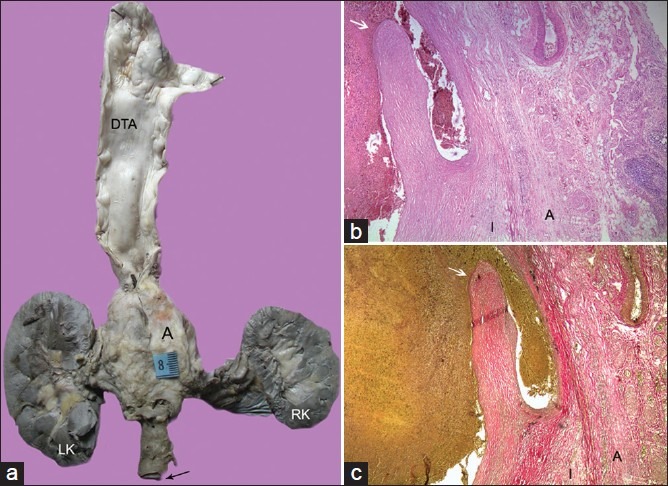
Scanned images of the ascending aorta, arch, left subclavian artery, descending thoracic aorta (elastic van Gieson), and abdominal aorta (Hematoxylin and Eosin, and elastic van Gieson) in a diffuse pattern of TA. All segments show marked adventitial fibrosis, the major cause of wall thickening. Lymph nodes (arrows) are seen around abdominal aorta
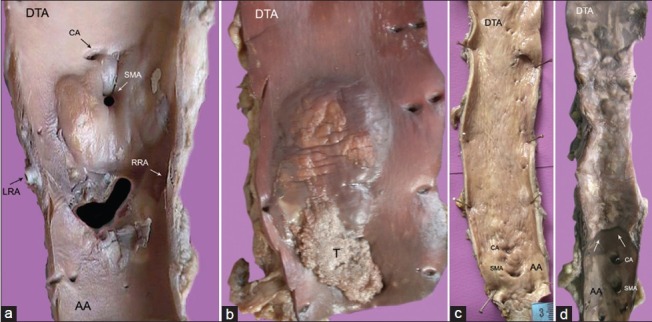
(a) Abdominal aorta with large, glistening intimal plaques seen around the superior mesenteric (SMA) and left (LRA), right (RRA) renal arteries; (b) single large gelatinous plaque with superimposed thrombosis (t) in descending thoracic aorta (DTA); (c) diffuse intimal thickening with superficial scars and furrows of entire descending aorta; (d) the localized disease affecting the descending thoracic aorta (DTA) is abruptly separated from normal abdominal aorta (AA) by a distinct shelf of intimal thickening

Cobble-stoned intima with atherosclerosis, calcification, and focal ulceration in an excised segment of ectatic descending aorta
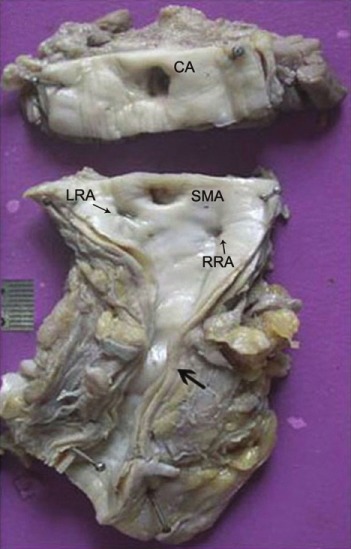
Intimal thickening of the abdominal aorta with extensive adventitial/peri-adventitial fibrosis and adherent adipose tissue. Note the presence of narrowing of the aortic lumen in the infra-renal region, and renal arterial ostia (CA, celiac artery; SMA, superior mesenteric artery; RRA, right renal artery; LRA, left renal artery)
(a) Multi-focal aortic disease with skip areas showing a large aneurysm in the abdominal aorta. The wall of the aneurysm when studied histologically also showed the presence of chronic dissection as seen in (b) (Hematoxylin and Eosin, ×100) and (c) (Elastic van Gieson, ×100). Arrow points to the intimal flap. The wall is represented only by thickened intima (I) and adventitia (A)
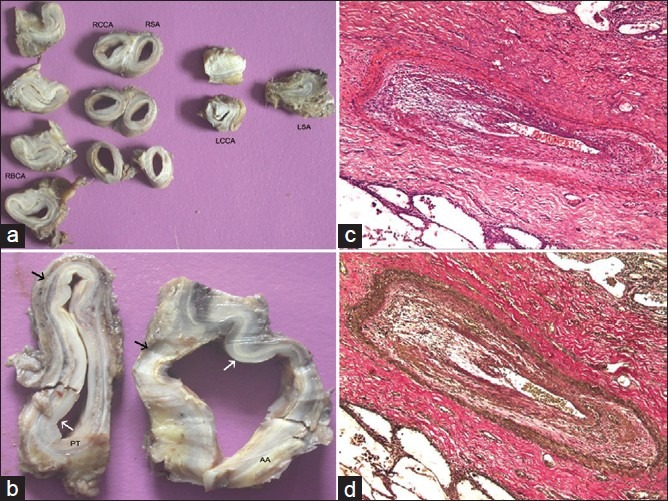
(a) There is involvement of all the arch arteries. Luminal obliteration is present in left common carotid artery (LCCA) and left subclavian artery (RBCA, right brachiocephalic artery; RCCA, right common carotid artery; RSA, right subclaivan artery). (b) The involvement of ascending aorta (AA) and pulmonary trunk (PT) is comparable. There is prominent intimal (white arrow) and adventitial (black arrow) thickening; The case also showed inflammation of the segmental branches seen in (c) (Hematoxylin and Eosin, ×250) and (d) (Elastic van Gieson, ×250)
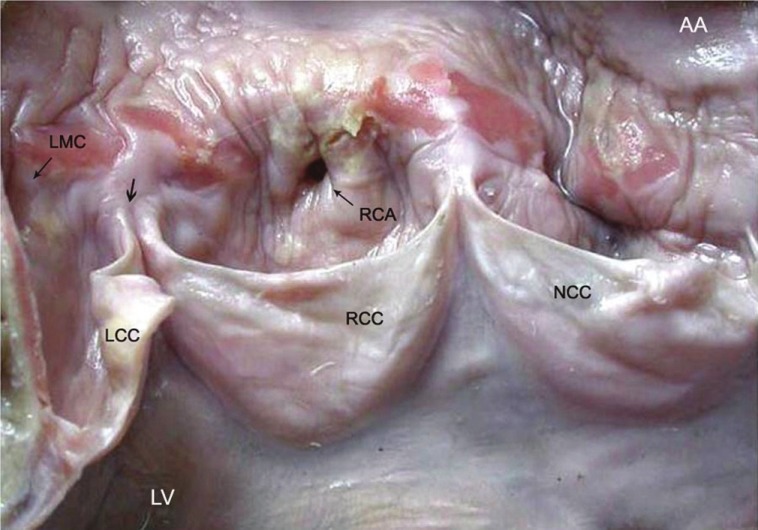
A 21-year-old woman, who presented with sudden cardiac death, showed TA manifesting as a band of aortitis affecting the ascending aorta (AA) with narrowing (thin arrow) of the dominant right coronary arterial (RCA) ostium. There is widening of the commissure (thick arrow) between right RCC and left LCC coronary cusps (LV, left ventricle; NCC, non-coronary cusp, LMC, left main coronary ostium)
References
-
- Jennette JC, Falk RJ, Bacon PA, Basu N, Cid MC, Ferrario F, et al. 2012 revised international chapel hill consensus conference nomenclature of vasculitides. Arthritis Rheum. 2013;65:1–11. - PubMed
-
- Luqmani R. Large vessel vasculitides: Update for the cardiologist. Curr Opin Cardiol. 2012;27:578–84. - PubMed
-
- Richards BL, March L, Gabriel SE. Epidemiology of large-vessel vasculitides. Best Pract Res Clin Rheumatol. 2010;24:871–3. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
