

Case Reports
doi: 10.1159/000348715.
Print 2013 Jan.
Advanced hepatocellular carcinoma in adolescence associated with congenital cholestasis: a case description
Affiliations
- PMID: 23626552
- PMCID: PMC3617980
- DOI: 10.1159/000348715
Item in Clipboard
Case Reports
Advanced hepatocellular carcinoma in adolescence associated with congenital cholestasis: a case description
Case Rep Oncol.
.
Abstract
This case describes the clinical course and treatment of a 17-year-old male patient with advanced hepatocellular carcinoma (HCC) arising in a non-cirrhotic liver. The disease was thought to be caused by a congenital cholestatic syndrome associated with intermittent oedema in childhood, resembling the rare Aagenaes syndrome. Treatment choices in advanced HCC arising in adolescence are discussed.
Keywords: Adolescence; Chemotherapy; Congenital cholestasis syndrome; Hepatocellular carcinoma; Juvenile; Treatment.
Figures
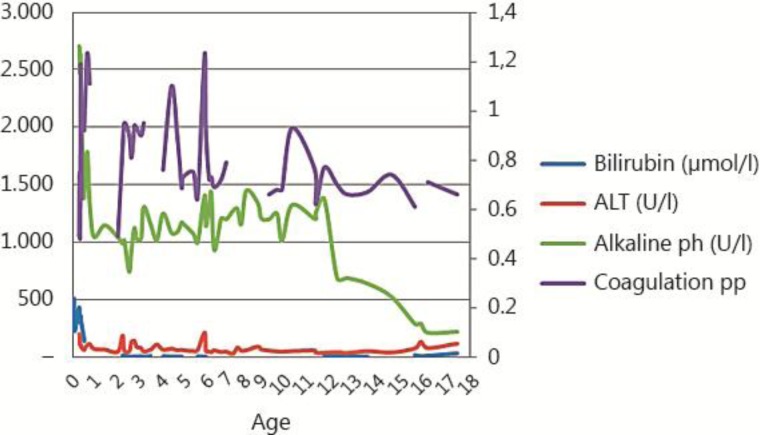
Liver function blood tests according to the patient's age. Bilirubin, ALT (alanine aminotransferase) and Alkaline ph (alkaline phosphatase) with units shown on left axis. Coagulation pp (prothrombin time) with units shown on right axis.
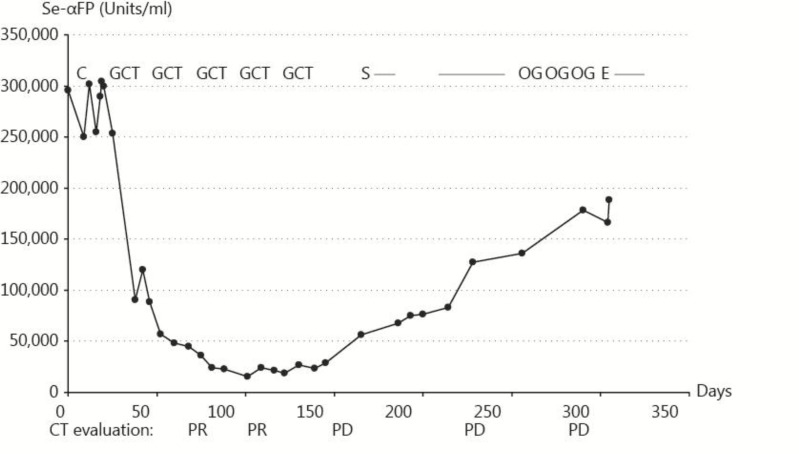
Serum α-foetoprotein (αFP) measured during treatment. Treatment schedules indicated: C = cisplatin 100 mg/m2 in a 3-week cycle; GCT = gemcitabine (G) 1,000 mg/m2 day 1 and 8, cisplatin (C) 70 mg/m2 day 1, and docetaxel (Taxol®, T) 175 mg/m2 day 1 in a 3-week cycle; S = sorafenib 400 mg p.o. b.i.d. reduced to 200 mg daily for 2 weeks after a 4-week break and then escalated to 400 mg daily; OG = oxaliplatin (O) 85 mg/m2, and gemcitabine (G) 1,000 mg/m2 every 2nd week; E = erlotinib p.o. 100 mg daily. Indicated below the x-axis are the results of tumour measurements by RECIST ver. 1.1. PR = Partial response; PD = progressive disease.
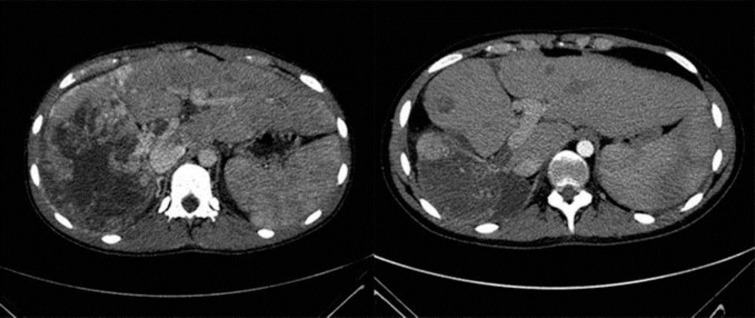
CT scans at baseline (left) and after six series of chemotherapy (right), showing a major partial response with shrinkage of the primary liver tumour.
References
-
- Czauderna P, Mackinlay G, Perilongo G, Brown J, Shafford E, Aronson D, Pritchard J, Chapchap P, Keeling J, Plaschkes J, Otte JB, Liver Tumors Study Group of the International Society of Pediatric Oncology Hepatocellular carcinoma in children: results of the first prospective study of the International Society of Pediatric Oncology group. J Clin Oncol. 2002;20:2798–2804. - PubMed
-
- Cruz O, Laguna A, Vancells M, Krauel L, Medina M, Mora J. Fibrolamellar hepatocellular carcinoma in an infant and literature review. J Ped Hematol Oncol. 2008;30:968–971. - PubMed
-
- Drivdal M, Trydal T, Hagve TA, Bergstad I, Aagenaes O. Prognosis, with evaluation of general biochemistry, of liver disease in lymphoedema cholestasis syndrome 1 (LCS1/Aagenaes syndrome) Scand J Gastroenterol. 2006;41:465–471. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
