

Distinct modulation of event-related potentials during motor preparation in patients with motor conversion disorder
- PMID: 23626829
- PMCID: PMC3633887
- DOI: 10.1371/journal.pone.0062539
Distinct modulation of event-related potentials during motor preparation in patients with motor conversion disorder
Abstract
Objective: Conversion paresis patients and healthy people feigning weakness both exhibit weak voluntary movement without detectable neuropathology. Uniquely, conversion patients lack a sense of conscious awareness of the origin of their impairment. We investigated whether conversion paresis patients show distinct electroencephalographic (EEG) markers associated with their unconscious movement deficits.
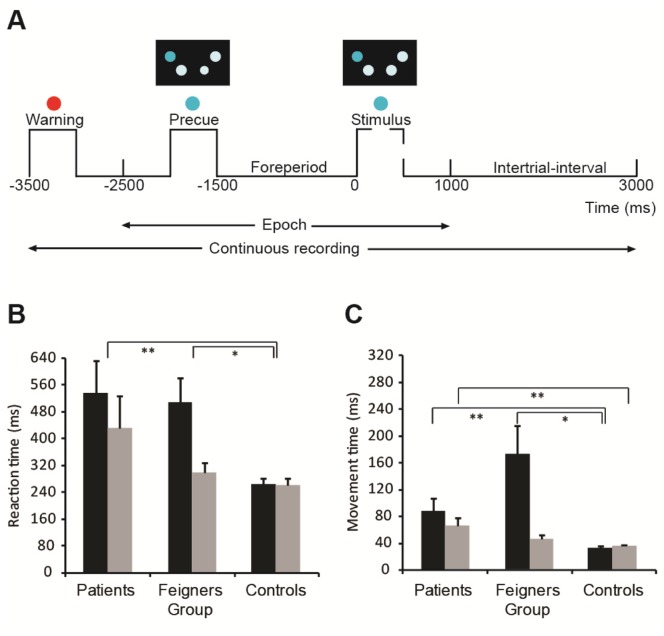
Methods: Six unilateral upper limb conversion paresis patients, 12 feigning participants asked to mimic weakness and 12 control participants performed a precued reaction time task, requiring movements of either hand, depending on precue information. Performance measures (force, reaction and movement time), and event-related EEG potentials (ERP) were compared, between groups and across hands or hemisphere, using linear mixed models.
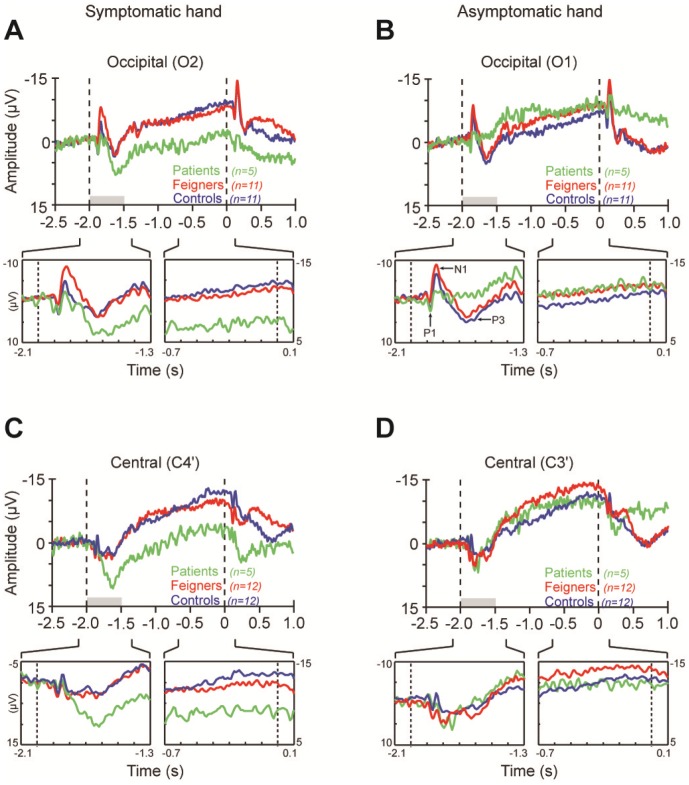
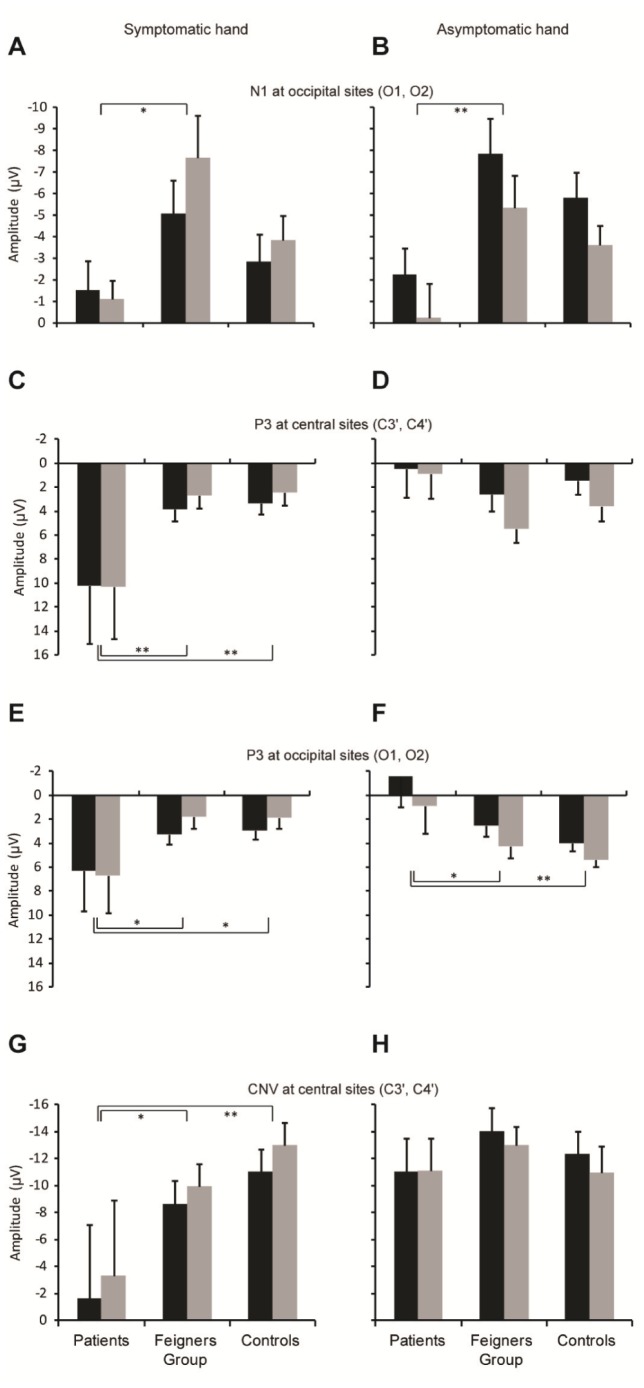
Results: Feigners generated the same inter-hand difference in reaction and movement time as expressed by patients, even though no specific targets were set nor feedback given on these measures. We found novel ERP signatures specific to patients. When the symptomatic hand was precued, the P3 ERP component accompanying the precue was dramatically larger in patients than in feigning participants. Additionally, in patients the earlier N1 ERP component was diminished when the precue signalled either the symptomatic or asymptomatic hand.
Conclusions: These results are consistent with previous suggestions that lack of awareness of the origin of their symptoms in conversion disorder patients may result from suppression of brain activity normally related to self-agency. In patients the diminished N1 to all precues is consistent with a generalised reduction in cognitive processing of movement-related precues. The P3 enhancement in patients is unlikely to simply reflect changes required for generation of impaired movements, because it was not seen in feigners showing the same behavioural deficits. Rather, this P3 enhancement in patients may represent a neural biomarker of unconscious processes, including additional emotional loading, related to active suppression of brain circuits involved in the attribution of self-agency.
Conflict of interest statement
Figures
Similar articles
-
Deficit in late-stage contingent negative variation provides evidence for disrupted movement preparation in patients with conversion paresis.Biol Psychol. 2015 Jul;109:73-85. doi: 10.1016/j.biopsycho.2015.04.009. Epub 2015 May 4. Biol Psychol. 2015. PMID: 25951783
-
Functional networks of motor inhibition in conversion disorder patients and feigning subjects.Neuroimage Clin. 2016 May 17;11:719-727. doi: 10.1016/j.nicl.2016.05.009. eCollection 2016. Neuroimage Clin. 2016. PMID: 27330971 Free PMC article.
-
Responses to cued signals in Parkinson's disease. Distinguishing between disorders of cognition and of activation.Brain. 1997 Aug;120 ( Pt 8):1355-75. doi: 10.1093/brain/120.8.1355. Brain. 1997. PMID: 9278628
-
Hysterical conversion and brain function.Prog Brain Res. 2005;150:309-29. doi: 10.1016/S0079-6123(05)50023-2. Prog Brain Res. 2005. PMID: 16186033 Review.
-
Neural correlates of motor conversion disorder.Motor Control. 2009 Apr;13(2):161-84. doi: 10.1123/mcj.13.2.161. Motor Control. 2009. PMID: 19454778 Review.
Cited by
-
Neural correlates of conversion disorder: overview and meta-analysis of neuroimaging studies on motor conversion disorder.BMC Psychiatry. 2016 Jun 10;16:195. doi: 10.1186/s12888-016-0890-x. BMC Psychiatry. 2016. PMID: 27283002 Free PMC article. Review.
-
Caloric vestibular stimulation as a treatment for conversion disorder: a case report and medical hypothesis.Front Psychiatry. 2014 Jun 2;5:63. doi: 10.3389/fpsyt.2014.00063. eCollection 2014. Front Psychiatry. 2014. PMID: 24917828 Free PMC article.
-
Uncovering the etiology of conversion disorder: insights from functional neuroimaging.Neuropsychiatr Dis Treat. 2016 Jan 13;12:143-53. doi: 10.2147/NDT.S65880. eCollection 2016. Neuropsychiatr Dis Treat. 2016. PMID: 26834476 Free PMC article. Review.
-
Blood CRP levels are elevated in children and adolescents with functional neurological symptom disorder.Eur Child Adolesc Psychiatry. 2019 Apr;28(4):491-504. doi: 10.1007/s00787-018-1212-2. Epub 2018 Aug 24. Eur Child Adolesc Psychiatry. 2019. PMID: 30143887
References
-
- American Psychiatric Association (1994) Diagnostic and Statistical Manual of Mental Disorders. Washington, DC: APA.
-
- Scott RL, Anson JG (2009) Neural correlates of motor conversion disorder. Motor Control 13: 161–184. - PubMed
-
- Tiihonen J, Kuikka J, Viinamäki H, Lehtonen J, Partanen J (1995) Altered cerebral blood flow during hysterical paresthesia. Biological Psychiatry 37: 134–135. - PubMed
-
- Vuilleumier P, Chicherio C, Assal F, Schwartz S, Slosman D, et al. (2001) Functional neuroanatomical correlates of hysterical sensorimotor loss. Brain 124: 1077–1090. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
