

Terminating ventricular tachyarrhythmias using far-field low-voltage stimuli: mechanisms and delivery protocols
- PMID: 23628521
- PMCID: PMC3735828
- DOI: 10.1016/j.hrthm.2013.04.027
Terminating ventricular tachyarrhythmias using far-field low-voltage stimuli: mechanisms and delivery protocols
Abstract
Background: Low-voltage termination of ventricular tachycardia (VT) and atrial fibrillation has shown promising results; however, the mechanisms and full range of applications remain unexplored.
Objectives: To elucidate the mechanisms for low-voltage cardioversion and defibrillation and to develop an optimal low-voltage defibrillation protocol.
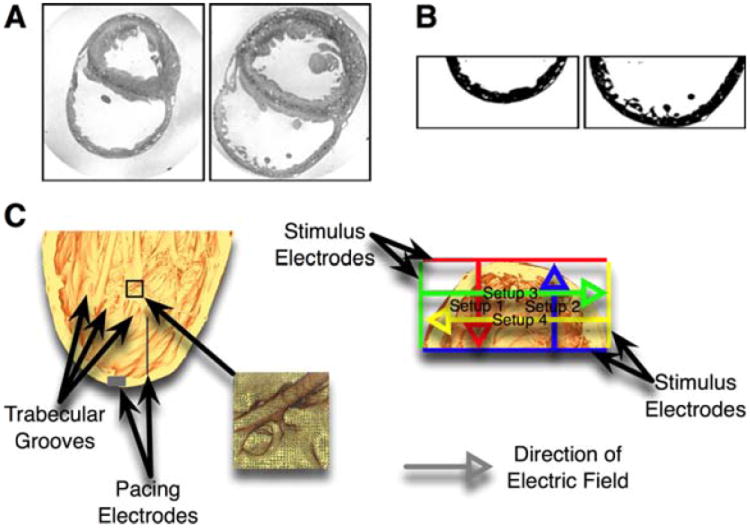
Methods: We developed a detailed magnetic resonance imaging-based computational model of the rabbit right ventricular wall. We applied multiple low-voltage far-field stimuli of various strengths (≤1 V/cm) and stimulation rates in VT and ventricular fibrillation (VF).
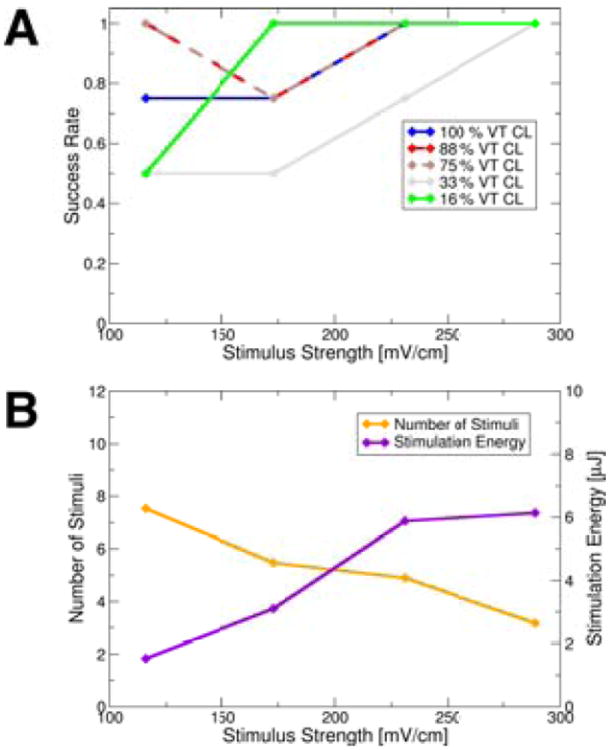
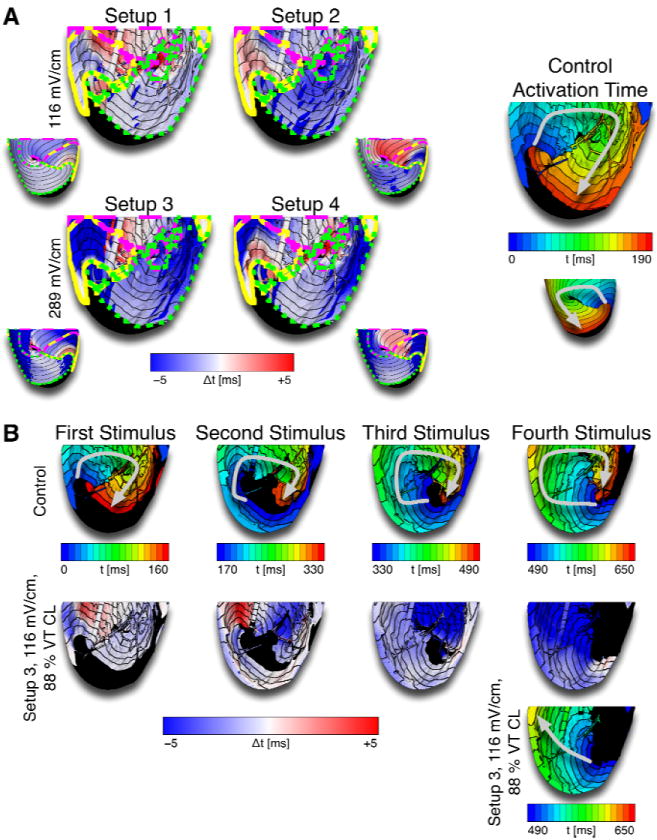
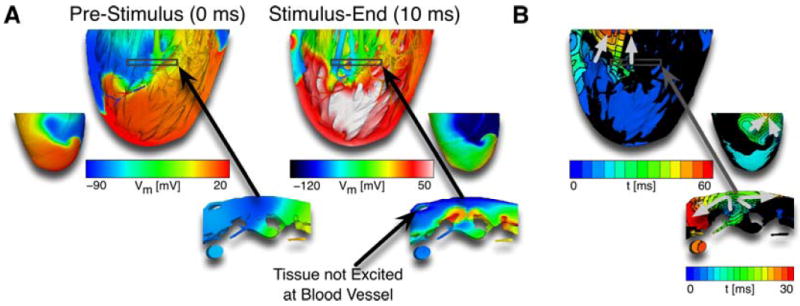
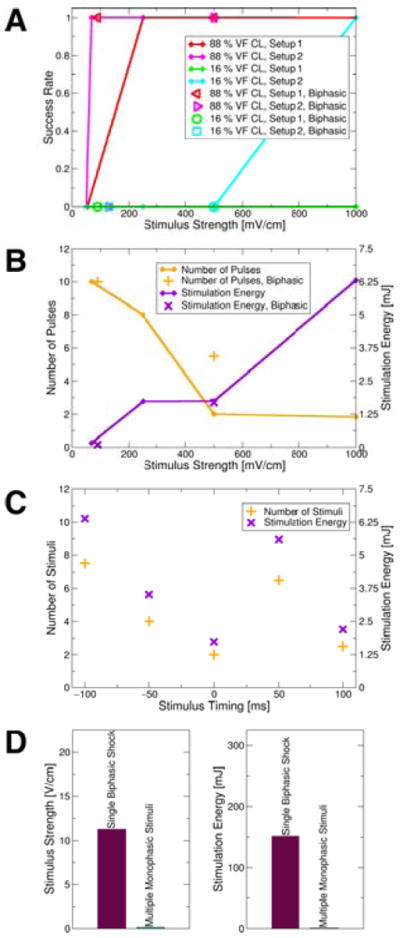
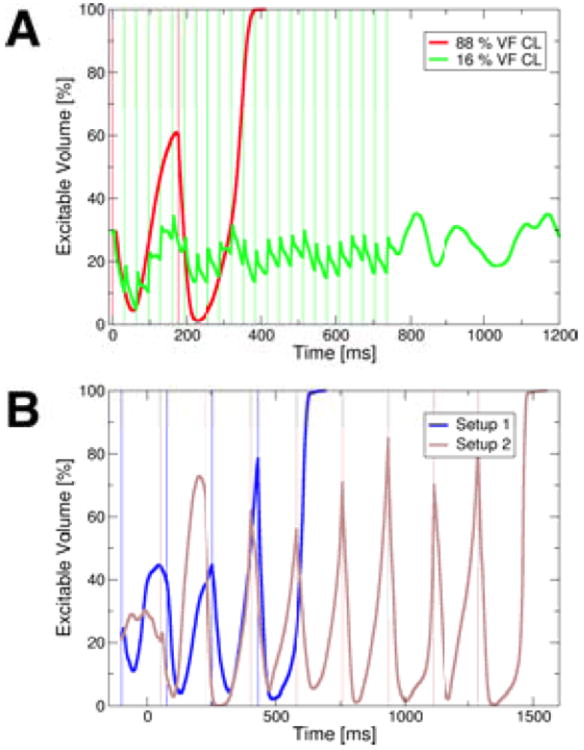
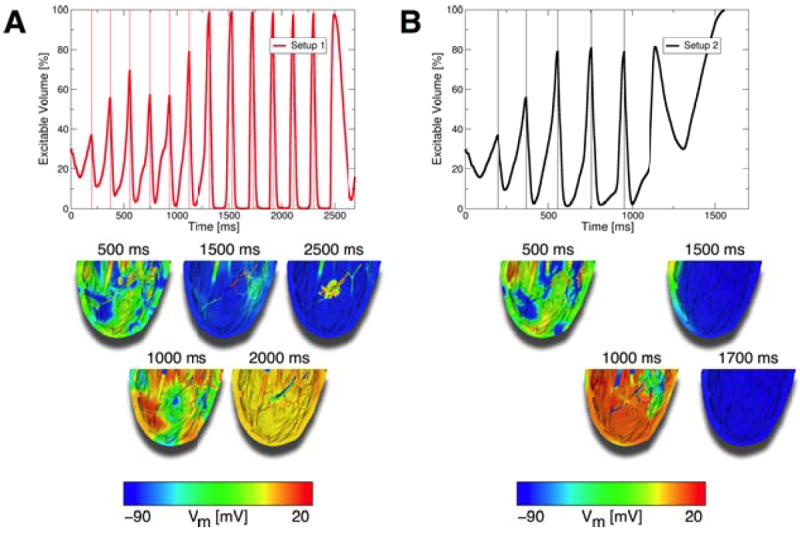
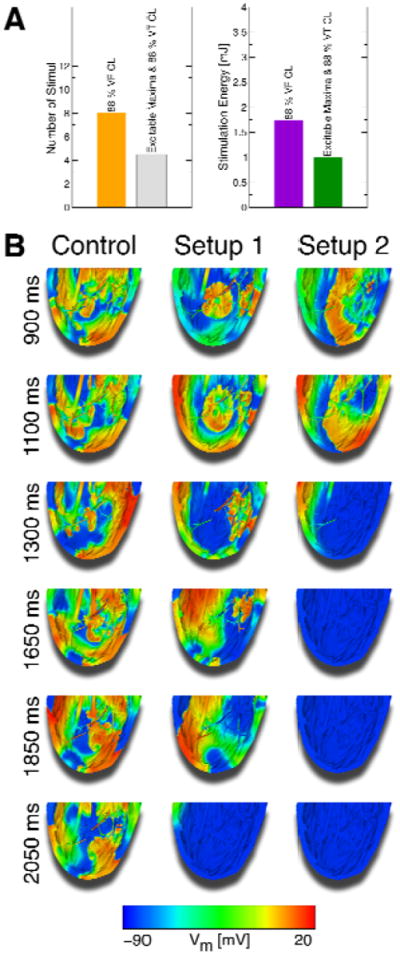
Results: Of the 5 stimulation rates tested, stimuli applied at 16% or 88% of the VT cycle length (CL) were most effective in cardioverting VT, the mechanism being consecutive excitable gap decreases. Stimuli given at 88% of the VF CL defibrillated successfully, whereas a faster stimulation rate (16%) often failed because the fast stimuli did not capture enough tissue. In this model, defibrillation threshold energy for multiple low-voltage stimuli at 88% of VF CL was 0.58% of the defibrillation threshold energy for a single strong biphasic shock. Based on the simulation results, a novel 2-stage defibrillation protocol was proposed. The first stage converted VF into VT by applying low-voltage stimuli at times of maximal excitable gap, capturing large tissue volume and synchronizing depolarization; the second stage terminated VT. The energy required for successful defibrillation using this protocol was 57.42% of the energy for low-voltage defibrillation when stimulating at 88% of VF CL.
Conclusions: A novel 2-stage low-voltage defibrillation protocol using the excitable gap extent to time multiple stimuli defibrillated VF with the least energy by first converting VF into VT and then terminating VT.
Keywords: AF; CL; Computer simulation; DFT; Electric countershock; Electric stimulation; RV; Tachycardia, Ventricular; V(m); VEP; VF; VT; Ventricular fibrillation; atrial fibrillation; cycle length; defibrillation threshold; extracellular potential; right ventricle/ventricular; transmembrane potential; ventricular fibrillation; ventricular tachycardia; virtual electrode polarization; Φ(e).
Copyright © 2013 Heart Rhythm Society. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
Bidomain simulations of defibrillation: 20 years of progress.Heart Rhythm. 2013 Aug;10(8):1218-9. doi: 10.1016/j.hrthm.2013.05.002. Epub 2013 May 2. Heart Rhythm. 2013. PMID: 23643512 No abstract available.
References
-
- Al-Khadra A, Nikolski V, Efimov IR. The role of electroporation in defibrillation. Circ Res. 2000 Oct 27;87:797–804. - PubMed
-
- Eysmann SB, Marchlinski FE, Buxton AE, Josephson ME. Electrocardiographic changes after cardioversion of ventricular arrhythmias. Circulation. 1986 Jan;73:73–81. - PubMed
-
- Tokano T, Bach D, Chang J, et al. Effect of ventricular shock strength on cardiac hemodynamics. J Cardiovasc Electrophysiol. 1998 Aug;9:791–797. - PubMed
-
- Larsen GK, Evans J, Lambert WE, Chen Y, Raitt MH. Shocks burden and increased mortality in implantable cardioverter-defibrillator patients. Heart Rhythm. 2011 Dec;8:1881–1886. - PubMed
-
- Maisel WH. Pacemaker and ICD generator reliability: meta-analysis of device registries. JAMA. 2006 Apr 26;295:1929–1934. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
