

Viral etiology of hospitalized acute lower respiratory infections in children under 5 years of age -- a systematic review and meta-analysis
- PMID: 23630140
- PMCID: PMC3641872
- DOI: 10.3325/cmj.2013.54.122
Viral etiology of hospitalized acute lower respiratory infections in children under 5 years of age -- a systematic review and meta-analysis
Abstract
Aim: To estimate the proportional contribution of influenza viruses (IV), parainfluenza viruses (PIV), adenoviruses (AV), and coronaviruses (CV) to the burden of severe acute lower respiratory infections (ALRI).
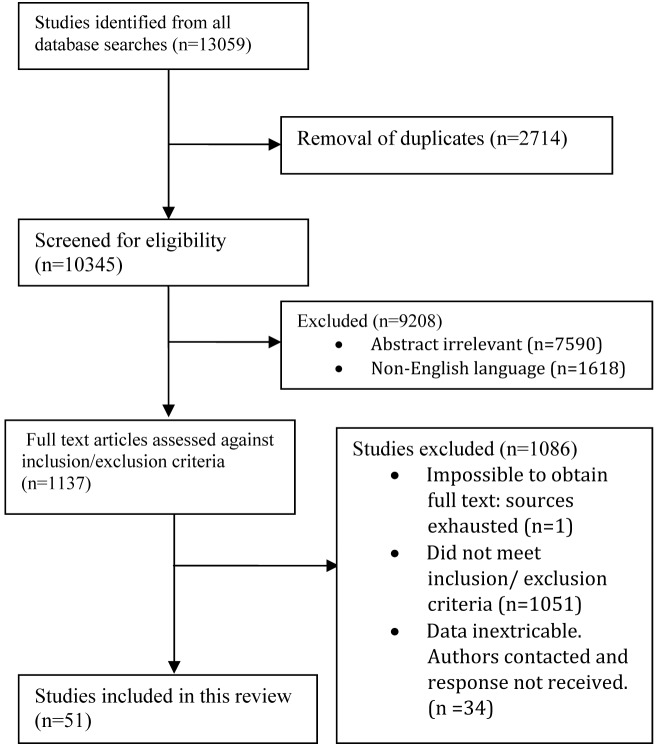
Methods: The review of the literature followed PRISMA guidelines. We included studies of hospitalized children aged 0-4 years with confirmed ALRI published between 1995 and 2011. A total of 51 studies were included in the final review, comprising 56091 hospitalized ALRI episodes.
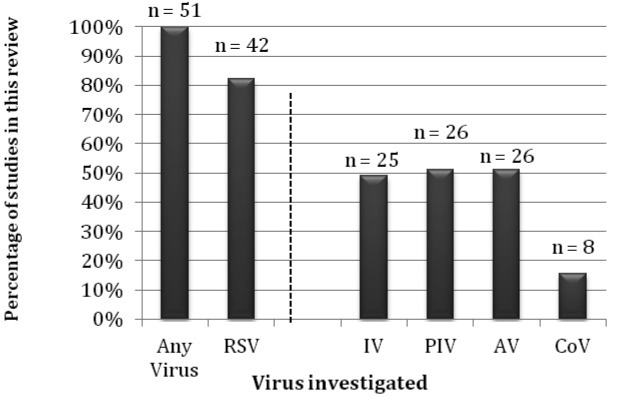
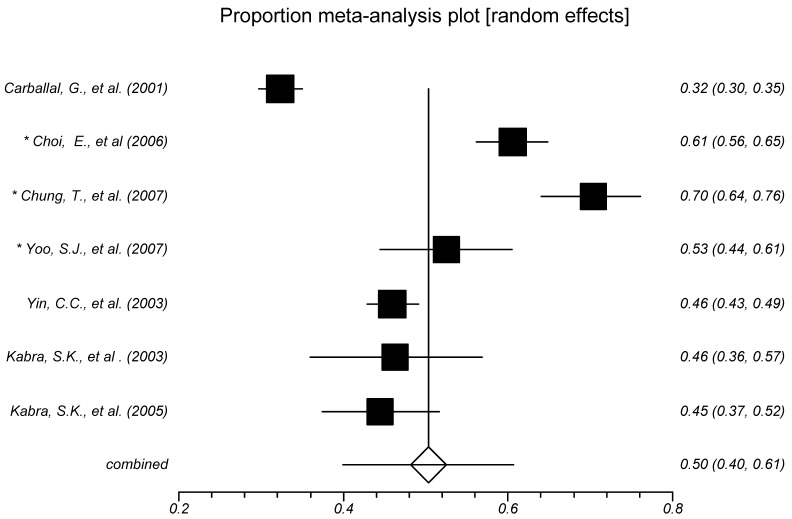
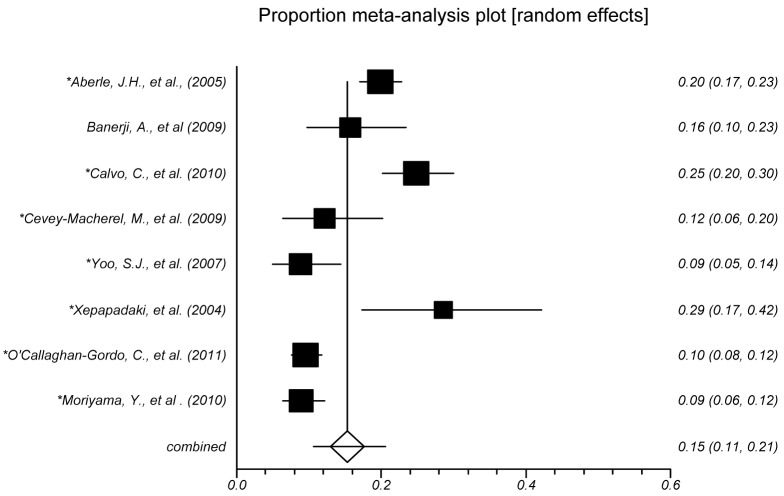
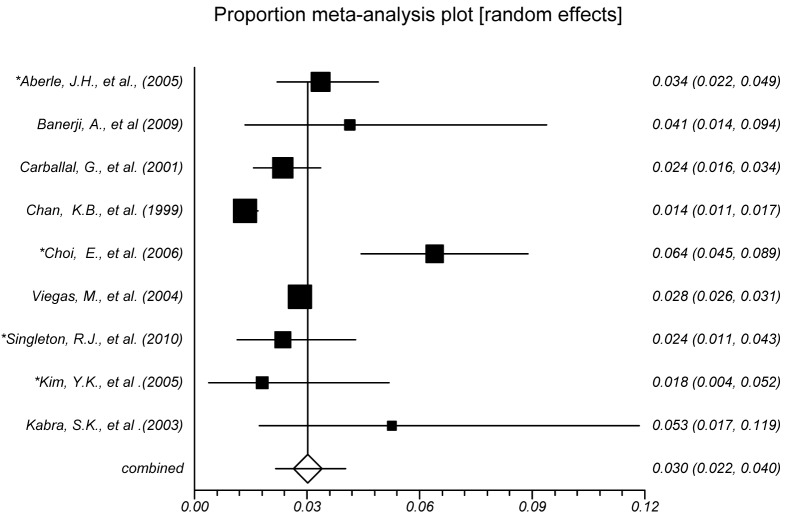
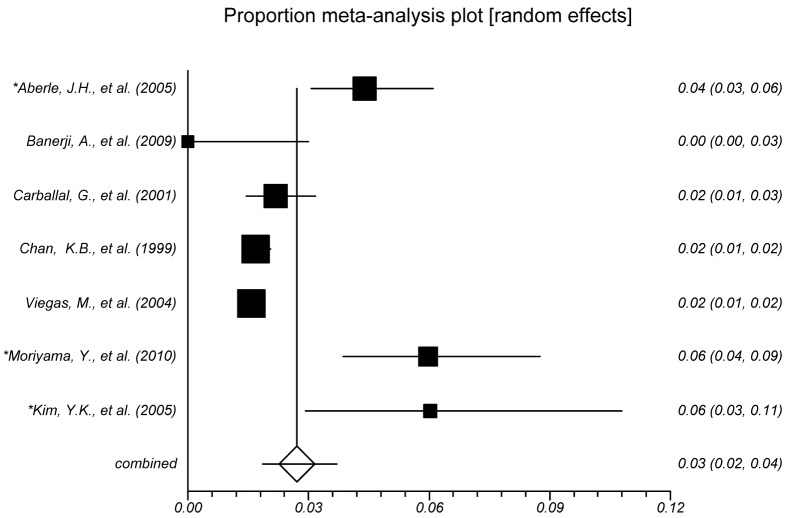
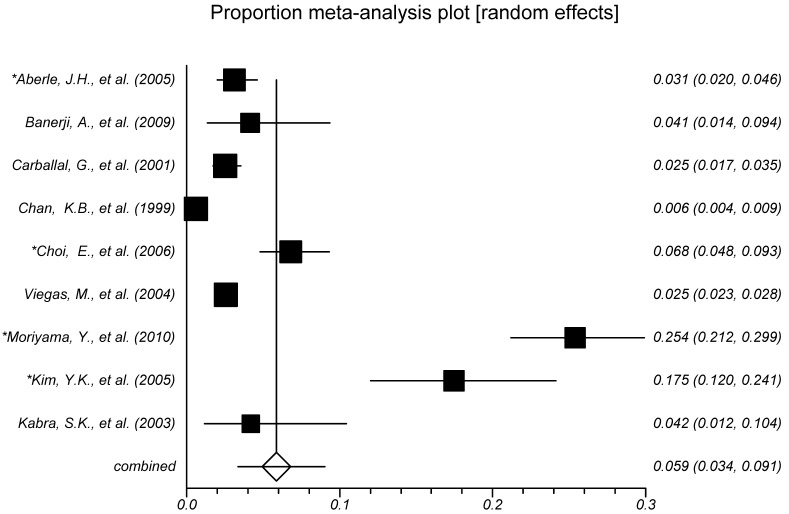
Results: IV was detected in 3.0% (2.2%-4.0%) of all hospitalized ALRI cases, PIV in 2.7% (1.9%-3.7%), and AV in 5.8% (3.4%-9.1%). CV are technically difficult to culture, and they were detected in 4.8% of all hospitalized ALRI patients in one study. When respiratory syncytial virus (RSV) and less common viruses were included, at least one virus was detected in 50.4% (40.0%-60.7%) of all hospitalized severe ALRI episodes. Moreover, 21.9% (17.7%-26.4%) of these viral ALRI were mixed, including more than one viral pathogen. Among all severe ALRI with confirmed viral etiology, IV accounted for 7.0% (5.5%-8.7%), PIV for 5.8% (4.1%-7.7%), and AV for 8.8% (5.3%-13.0%). CV was found in 10.6% of virus-positive pneumonia patients in one study.
Conclusions: This article provides the most comprehensive analysis of the contribution of four viral causes to severe ALRI to date. Our results can be used in further cost-effectiveness analyses of vaccine development and implementation for a number of respiratory viruses.
Figures
References
-
- Waters D, Theodoratou E, Campbell H, Rudan I, Chopra M. Optimizing community case management strategies to achieve equitable reduction of childhood pneumonia mortality: An application of Equitable Impact Sensitive Tool (EQUIST) in five low- and middle-income countries. J Glob Health. 2012;2:20402. doi: 10.7189/jogh.02.020402. - DOI - PMC - PubMed
-
- Seaton A, Seaton D, Leitch AG, editors. Crofton and Douglas's Respiratory Diseases. 5th ed. Oxford (UK): Blackwell Science Ltd; 2000.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources