

The outcome of prophylactic intravenous cefazolin and ceftriaxone in cirrhotic patients at different clinical stages of disease after endoscopic interventions for acute variceal hemorrhage
- PMID: 23630607
- PMCID: PMC3632526
- DOI: 10.1371/journal.pone.0061666
The outcome of prophylactic intravenous cefazolin and ceftriaxone in cirrhotic patients at different clinical stages of disease after endoscopic interventions for acute variceal hemorrhage
Abstract
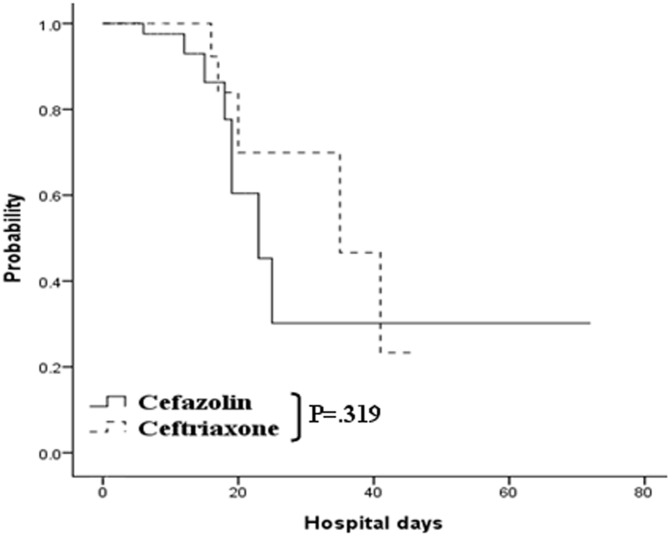
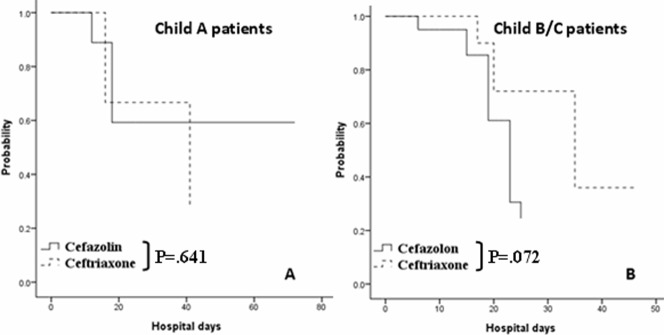
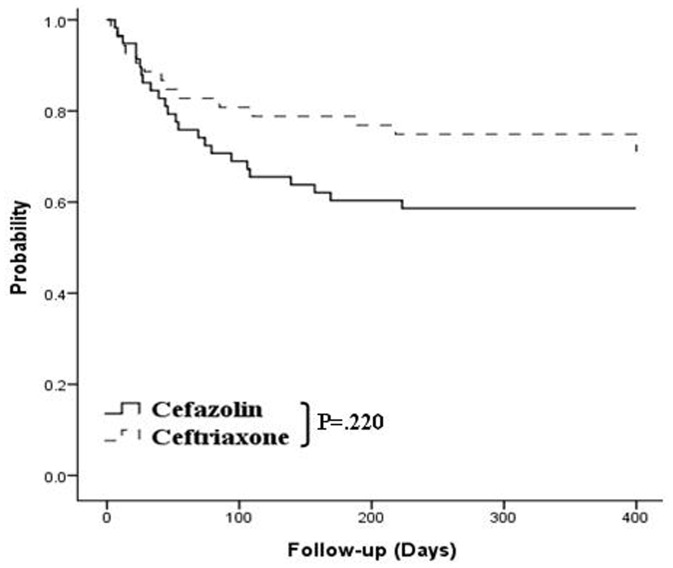
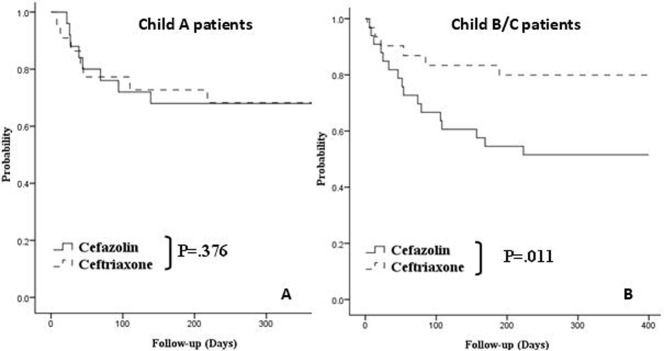
Antibiotic prophylaxis with norfloxacin, intravenous ciprofloxacin, or ceftriaxone has been recommended for cirrhotic patients with gastrointestinal hemorrhage but little is known about intravenous cefazolin. This study aimed to compare the outcome of intravenous cefazolin and ceftriaxone as prophylactic antibiotics among cirrhotic patients at different clinical stages, and to identify the associated risk factors. The medical records of 713 patients with acute variceal bleeding who had received endoscopic procedures from were reviewed. Three hundred and eleven patients were entered for age-matched adjustment after strict exclusion criteria. After the adjustment, a total of 102 patients were enrolled and sorted into 2 groups according to the severity of cirrhosis: group A (Child's A patients, n = 51) and group B (Child's B and C patients, n = 51). The outcomes were prevention of infection, time of rebleeding, and death. Our subgroup analysis results failed to show a significant difference in infection prevention between patients who received prophylactic cefazolin and those who received ceftriaxone among Child's A patients (93.1% vs. 90.9%, p = 0.641); however, a trend of significance in favor of ceftriaxone prophylaxis (77.8% vs. 87.5%, p = 0.072) was seen among Child's B and C patients. More rebleeding cases were observed in patients who received cefazolin than in those who received ceftriaxone among Child's B and C patients (66.7% vs. 25.0%, p = 0.011) but not in Child's A patients (32% vs. 40.9%, p = 0.376). The risk factors associated with rebleeding were history of bleeding and use of prophylactic cefazolin among Child's B and C patients. In conclusion, this study suggests that prophylactic intravenous cefazolin may not be inferior to ceftriaxone in preventing infections and reducing rebleeding among Child's A cirrhotic patients after endoscopic interventions for acute variceal bleeding. Prophylactic intravenous ceftriaxone yields better outcome among Child's B and C patients.
Conflict of interest statement
Figures
References
-
- Rimola A, Bory F, Teres J, Perez-Ayuso RM, Arroyo V, et al. (1985) Oral, nonabsorbable antibiotics prevent infection in cirrhotics with gastrointestinal hemorrhage. Hepatology 5: 463–467. - PubMed
-
- Soriano G, Guarner C, Tomas A, Villanueva C, Torras X, et al. (1992) Norfloxacin prevents bacterial infection in cirrhotics with gastrointestinal hemorrhage. Gastroenterology 103: 1267–1272. - PubMed
-
- Pauwels A, Mostefa-Kara N, Debenes B, Degoutte E, Levy VG (1996) Systemic antibiotic prophylaxis after gastrointestinal hemorrhage in cirrhotic patients with a high risk of infection. Hepatology 24: 802–806. - PubMed
-
- Bernard B, Grange JD, Khac EN, Amiot X, Opolon P, et al. (1999) Antibiotic prophylaxis for the prevention of bacterial infections in cirrhotic patients with gastrointestinal bleeding: a meta-analysis. Hepatology 29: 1655–1661. - PubMed
-
- Fernandez J, Navasa M, Gomez J, Colmenero J, Vila J, et al. (2002) Bacterial infections in cirrhosis: epidemiological changes with invasive procedures and norfloxacin prophylaxis. Hepatology 35: 140–148. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
