

Role of circulating angiotensin converting enzyme 2 in left ventricular remodeling following myocardial infarction: a prospective controlled study
- PMID: 23630610
- PMCID: PMC3632515
- DOI: 10.1371/journal.pone.0061695
Role of circulating angiotensin converting enzyme 2 in left ventricular remodeling following myocardial infarction: a prospective controlled study
Abstract
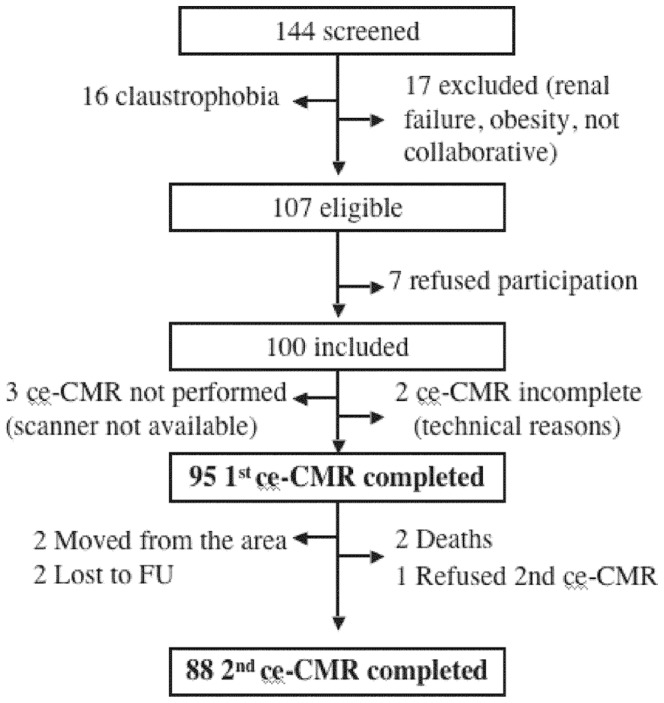
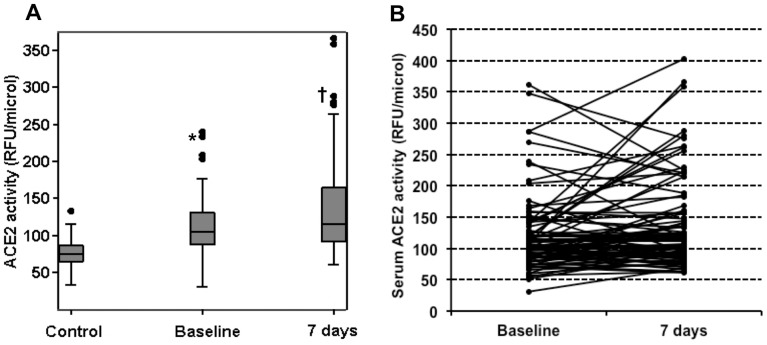
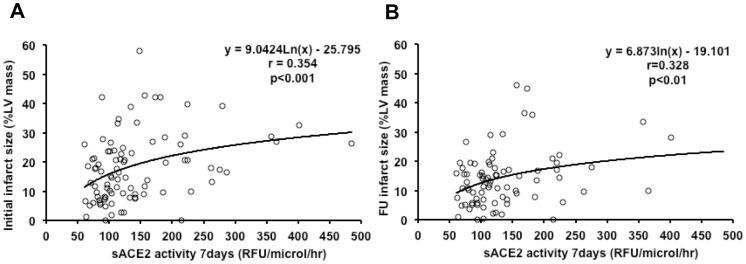
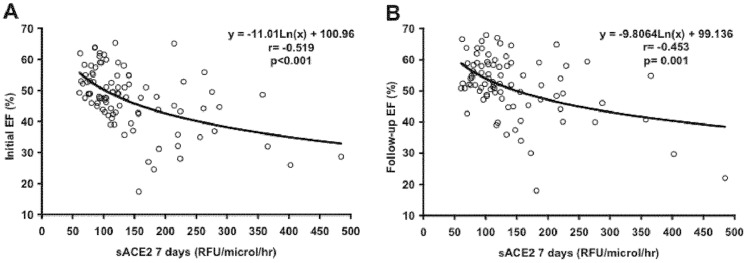
Angiotensin-converting enzyme 2 (ACE2) cleaves Angiotensin-II to Angiotensin-(1-7), a cardioprotective peptide. Serum soluble ACE2 (sACE2) activity is raised in chronic heart failure, suggesting a compensatory role in left ventricular dysfunction. Our aim was to study the relationship between sACE2 activity, infarct size, left ventricular systolic function and remodeling following ST-elevation myocardial infarction (STEMI). A contrast-enhanced cardiac magnetic resonance study was performed acutely in 95 patients with first STEMI and repeated at 6 months to measure LV end-diastolic volume index, ejection fraction and infarct size. Baseline sACE2 activities, measured by fluorescent enzymatic assay 24 to 48 hours and at 7 days from admission, were compared to that obtained in 22 matched controls. Patients showed higher sACE2 at baseline than controls (104.4 [87.4-134.8] vs 74.9 [62.8-87.5] RFU/µl/hr, p<0.001). At seven days, sACE2 activity significantly increased from baseline (115.5 [92.9-168.6] RFU/µl/hr, p<0.01). An inverse correlation between sACE2 activity with acute and follow-up ejection fraction was observed (r = -0.519, p<0.001; r = -0.453, p = 0.001, respectively). Additionally, sACE2 directly correlated with infarct size (r = 0.373, p<0.001). Both, infarct size (β = -0.470 [95%CI:-0.691:-0.248], p<0.001) and sACE2 at 7 days (β = -0.025 [95%CI:-0.048:-0.002], p = 0.030) were independent predictors of follow-up ejection fraction. Patients with sACE2 in the upper tertile had a 4.4 fold increase in the incidence of adverse left ventricular remodeling (95% confidence interval: 1.3 to 15.2, p = 0.027). In conclusion, serum sACE2 activity rises in relation to infarct size, left ventricular systolic dysfunction and is associated with the occurrence of left ventricular remodeling.
Conflict of interest statement
Figures
References
-
- Pfeffer MA, McMurray JJ, Velazquez EJ, Rouleau JL, Kober L, et al. (2003) Valsartan, captopril, or both in myocardial infarction complicated by heart failure, left ventricular dysfunction, or both. N Engl J Med 349: 1893–1906. - PubMed
-
- Pitt B, Remme W, Zannad F, Neaton J, Martinez F, et al. (2003) Eplerenone, a selective aldosterone blocker, in patients with left ventricular dysfunction after myocardial infarction. N Engl J Med 348: 1309–1321. - PubMed
-
- Wu E, Ortiz JT, Tejedor P, Lee DC, Bucciarelli-Ducci C, et al. (2008) Infarct size by contrast enhanced cardiac magnetic resonance is a stronger predictor of outcomes than left ventricular ejection fraction or end-systolic volume index: prospective cohort study. Heart 94: 730–736. - PubMed
-
- Loot AE, Roks AJ, Henning RH, Tio RA, Suurmeijer AJ, et al. (2002) Angiotensin-(1–7) attenuates the development of heart failure after myocardial infarction in rats. Circulation 105: 1548–1550. - PubMed
-
- Crackower MA, Sarao R, Oudit GY, Yagil C, Kozieradzki I, et al. (2002) Angiotensin-converting enzyme 2 is an essential regulator of heart function. Nature 417: 822–828. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
