

Risk factors for postoperative hypoxemia in patients undergoing Stanford A aortic dissection surgery
- PMID: 23631417
- PMCID: PMC3649943
- DOI: 10.1186/1749-8090-8-118
Risk factors for postoperative hypoxemia in patients undergoing Stanford A aortic dissection surgery
Abstract
Background: The purpose of this study is to identify the risk factors for postoperative hypoxemia in patients with Stanford A aortic dissection surgery and their relation to clinical outcomes.
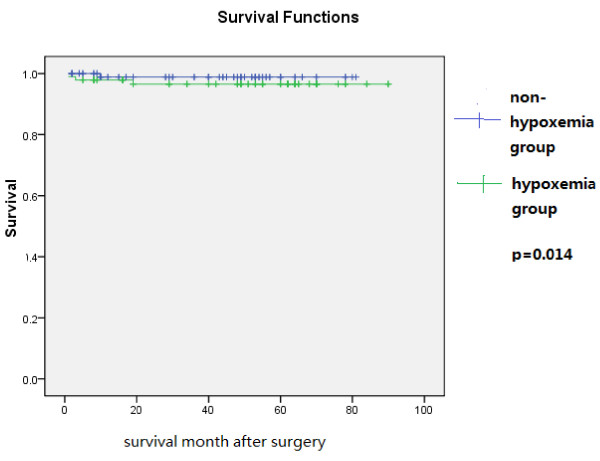
Methods: Clinical records of 186 patients with postoperative hypoxemia in Stanford A aortic dissection were analyzed retrospectively. The patients were divided into two groups by postoperative oxygen fraction (PaO2/FiO2):hypoxemia group (N=92) and non-hypoxemia group (N=94).
Results: We found that the incidence of postoperative hypoxemia was 49.5%. Statistical analysis by t-test and χ2 indicated that acute onset of the aortic dissection (p=0.000), preoperative oxygen fraction (PaO2/FiO2) ≤200 mmHg(p=0.000), body mass index (p=0.008), circulatory arrest (CA) time (p=0.000) and transfusion more than 3000 ml(p=0.000) were significantly associated with postoperative hypoxemia. Multiple logistic regression analysis showed that preoperative hypoxemia, CA time and transfusion more than 3000 ml were independently associated with postoperative hypoxemia in Stanford A aortic dissection.
Conclusion: Our results suggest that postoperative hypoxemia is a common complication in patients treated by Stanford A aortic dissection surgery. Preoperative oxygen fraction lower than 200 mmHg, longer CA time and transfusion more than 3000 ml are predictors of postoperative hypoxemia in Stanford A aortic dissection.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
