

Multicenter implementation of a severe sepsis and septic shock treatment bundle
- PMID: 23631750
- PMCID: PMC3735248
- DOI: 10.1164/rccm.201212-2199OC
Multicenter implementation of a severe sepsis and septic shock treatment bundle
Abstract
Rationale: Severe sepsis and septic shock are leading causes of intensive care unit (ICU) admission, morbidity, and mortality. The effect of compliance with sepsis management guidelines on outcomes is unclear.
Objectives: To assess the effect on mortality of compliance with a severe sepsis and septic shock management bundle.
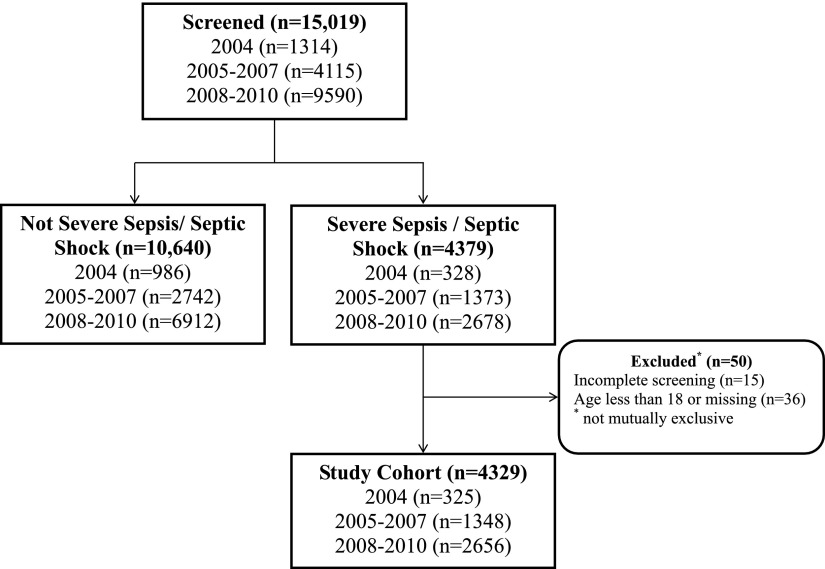
Methods: Observational study of a severe sepsis and septic shock bundle as part of a quality improvement project in 18 ICUs in 11 hospitals in Utah and Idaho.
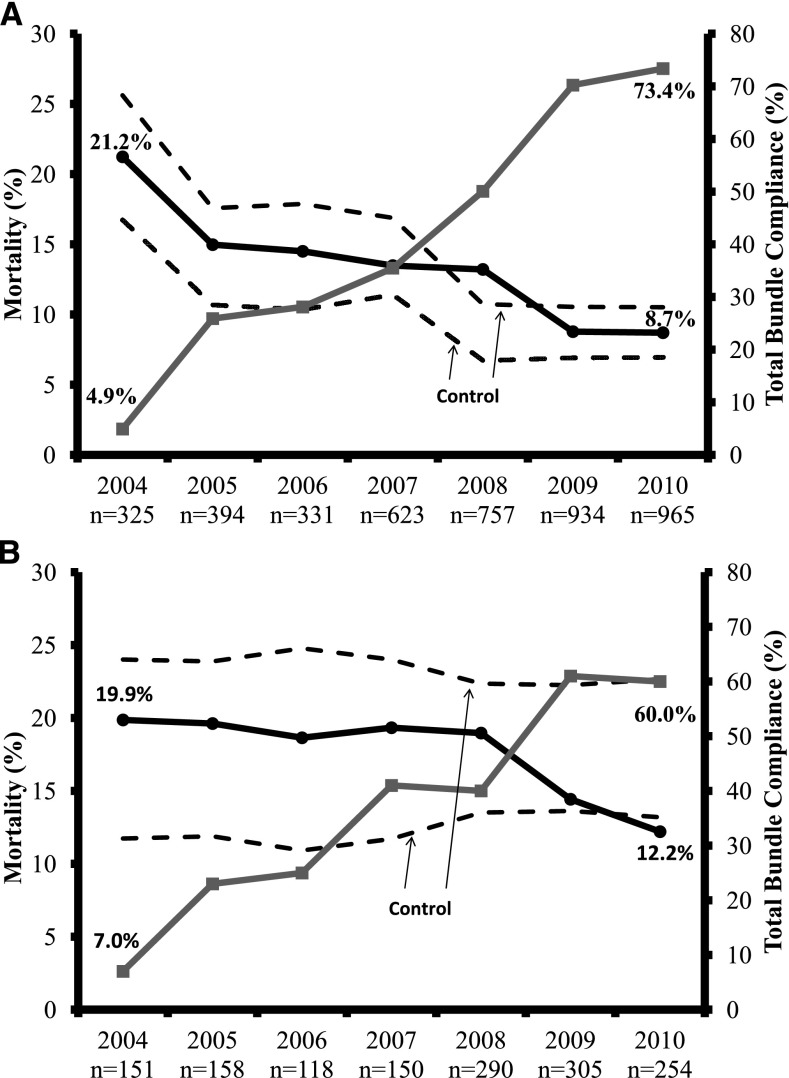
Measurements and main results: Among 4,329 adult subjects with severe sepsis or septic shock admitted to study ICUs from the emergency department between January 2004 and December 2010, hospital mortality was 12.1%, declining from 21.2% in 2004 to 8.7% in 2010. All-or-none total bundle compliance increased from 4.9-73.4% simultaneously. Mortality declined from 21.7% in 2004 to 9.7% in 2010 among subjects noncompliant with one or more bundle element. Regression models adjusting for age, severity of illness, and comorbidities identified an association between mortality and compliance with each of inotropes and red cell transfusions, glucocorticoids, and lung-protective ventilation. Compliance with early resuscitation elements during the first 3 hours after emergency department admission caused ineligibility, through lower subsequent severity of illness, for these later bundle elements.
Conclusions: Total severe sepsis and septic shock bundle compliances increased substantially and were associated with a marked reduction in hospital mortality after adjustment for age, severity of illness, and comorbidities in a multicenter ICU cohort. Early resuscitation bundle element compliance predicted ineligibility for subsequent bundle elements.
Figures
Comment in
-
Early recognition and treatment of severe sepsis.Am J Respir Crit Care Med. 2013 Jul 1;188(1):7-8. doi: 10.1164/rccm.201304-0801ED. Am J Respir Crit Care Med. 2013. PMID: 23815716 No abstract available.
References
-
- Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J, Pinsky MR. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med. 2001;29:1303–1310. - PubMed
-
- Martin GS, Mannino DM, Eaton S, Moss M. The epidemiology of sepsis in the United States from 1979 through 2000. N Engl J Med. 2003;348:1546–1554. - PubMed
-
- Bernard GR, Vincent JL, Laterre PF, LaRosa SP, Dhainaut JF, Lopez-Rodriguez A, Steingrub JS, Garber GE, Helterbrand JD, Ely EW, et al. Group RhpCWEiSSs. Efficacy and safety of recombinant human activated protein C for severe sepsis. N Engl J Med. 2001;344:699–709. - PubMed
-
- Annane D, Aegerter P, Jars-Guincestre MC, Guidet B. Network CU-R. Current epidemiology of septic shock: the CUB-REA network. Am J Respir Crit Care Med. 2003;168:165–172. - PubMed
-
- Dombrovskiy VY, Martin AA, Sunderram J, Paz HL. Rapid increase in hospitalization and mortality rates for severe sepsis in the United States: a trend analysis from 1993 to 2003. Crit Care Med. 2007;35:1244–1250. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
