

Association of serum phosphorus concentration with mortality in elderly and nonelderly hemodialysis patients
- PMID: 23631888
- PMCID: PMC3735629
- DOI: 10.1053/j.jrn.2013.01.018
Association of serum phosphorus concentration with mortality in elderly and nonelderly hemodialysis patients
Abstract
Objective: Hypo- and hyperphosphatemia have each been associated with increased mortality in maintenance hemodialysis (MHD) patients. There has not been previous evaluation of a differential relationship between serum phosphorus level and death risk across varying age groups in MHD patients.
Design and settings: In a 6-year cohort of 107,817 MHD patients treated in a large dialysis organization, we examined the association between serum phosphorus levels with all-cause and cardiovascular mortality within 5 age categories (15 to <45, 45 to <65, 65 to <70, 70 to <75, and ≥75 years old) using Cox proportional hazards models adjusted for case-mix covariates and malnutrition inflammation complex syndrome (MICS) surrogates.
Main outcome measure: All-cause and cardiovascular mortality.
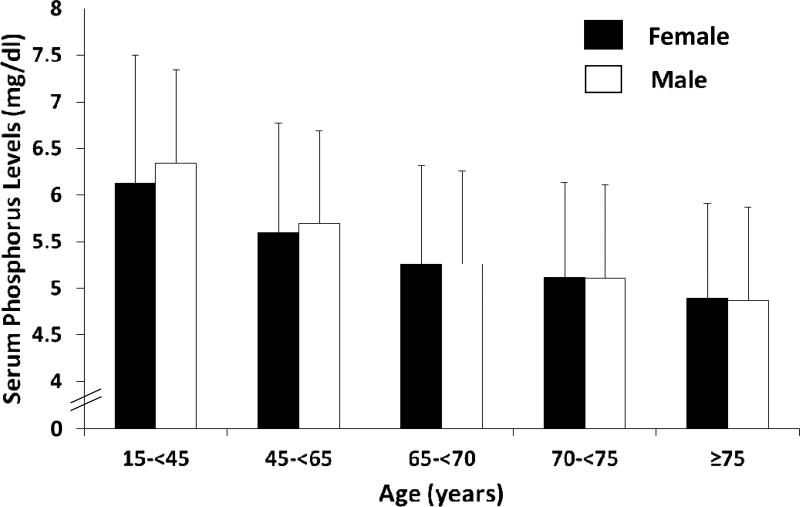
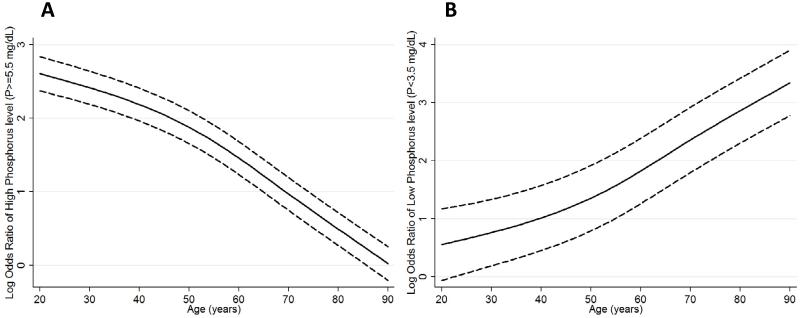
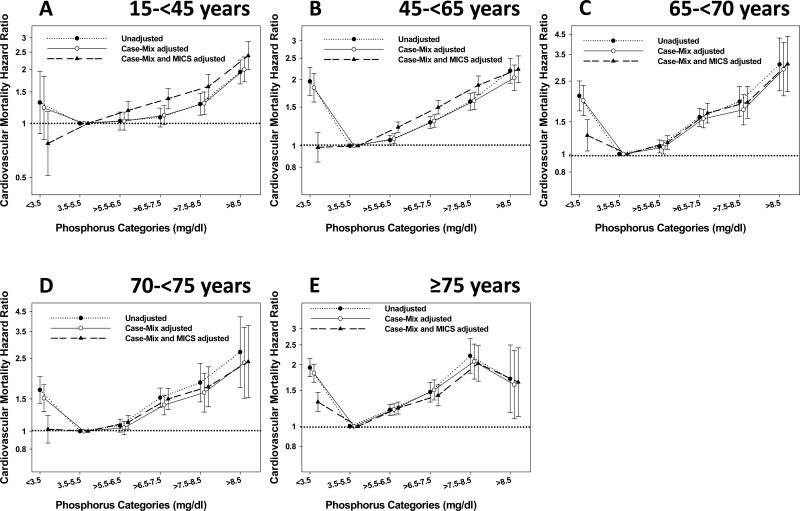
Results: The overall mean age of the cohort was 60 ± 16 years, among whom there were 45% women, 35% Blacks, and 58% diabetics. The time-averaged serum phosphorus level (mean ± SD) within each age category was 6.26 ± 1.4, 5.65 ± 1.2, 5.26 ± 1.1, 5.11 ± 1.0, and 4.88 ± 1.0 mg/dL, respectively (P for trend <.001). Hyperphosphatemia (>5.5 mg/dL) was consistently associated with increased all-cause and cardiovascular mortality risks across all age categories, including after adjustment for case-mix and MICS-related covariates. In fully adjusted models, a low serum phosphorus level (<3.5 mg/dL) was associated with increased all-cause mortality only in elderly MHD patients ≥65 years old (hazard ratio [95% confidence interval]: 1.21 [1.07-1.37], 1.13 [1.02-1.25], and 1.28 [1.2-1.37] for patients 65 to <70, 70 to <75, and ≥75 years old, respectively), but not in younger patients (<65 years old). A similar differential cardiovascular mortality risk for low serum phosphorus levels between old and young age groups was observed.
Conclusions: The association between hyperphosphatemia and mortality is similar across all age groups of MHD patients, whereas hypophosphatemia is associated with increased mortality only in elderly MHD patients. Preventing very low serum phosphorus levels in elderly dialysis patients may be associated with better outcomes, which needs to be examined in future studies.
Copyright © 2013 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Figures

References
-
- Foley RN, Parfrey PS, Sarnak MJ. Clinical epidemiology of cardiovascular disease in chronic renal disease. Am J Kidney Dis. 1998;32(5 Suppl 3):S112–S119. - PubMed
-
- Shoji T, Maekawa K, Emoto M, et al. Arterial stiffness predicts cardiovascular death independent of arterial thickness in a cohort of hemodialysis patients. Atherosclerosis. 2010;210(1):145–149. - PubMed
-
- Longenecker JC, Coresh J, Powe NR, et al. Traditional cardiovascular disease risk factors in dialysis patients compared with the general population: the CHOICE Study. J Am Soc Nephrol. 2002;13(7):1918–1927. - PubMed
-
- Sarnak MJ. Cardiovascular complications in chronic kidney disease. Am J Kidney Dis. 2003;41(6 Suppl 5):11–17. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
