

Analysis of the efficacy of portal vein embolization for patients with extensive liver malignancy and very low future liver remnant volume, including a comparison with the associating liver partition with portal vein ligation for staged hepatectomy approach
- PMID: 23632095
- PMCID: PMC3880191
- DOI: 10.1016/j.jamcollsurg.2013.03.004
Analysis of the efficacy of portal vein embolization for patients with extensive liver malignancy and very low future liver remnant volume, including a comparison with the associating liver partition with portal vein ligation for staged hepatectomy approach
Abstract
Background: The primary reported indication for the associating liver partition with portal vein ligation for staged hepatectomy (ALPPS) technique is in patients with very low future liver remnant volumes. Given the elevated incidence of major morbidity (40%) and liver-related mortality (12%) with ALPPS, we sought to determine the safety and efficacy of percutaneous portal vein embolization (PVE) in a similar patient population.
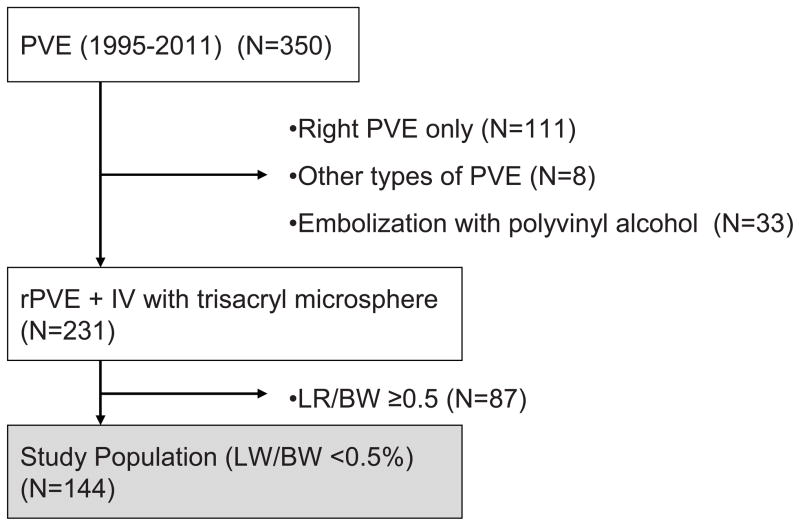
Study design: Tumor resectability and morbidity and mortality rates were reviewed for 144 consecutive liver tumor patients with future liver remnant to body weight ratios (LR/BW) less than 0.5%. All patients were referred for preoperative percutaneous right plus segment IV PVE using embolic microspheres, with planned reassessment of the LR/BW 30 days after PVE. Post-PVE outcomes were compared with reported outcomes for ALPPS.
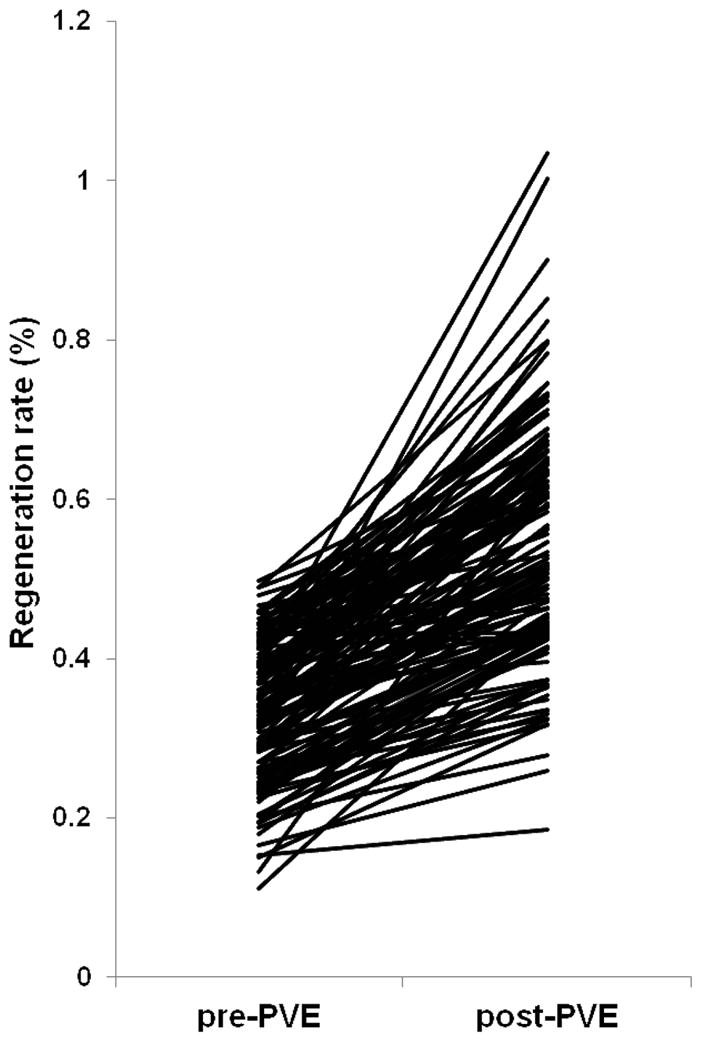
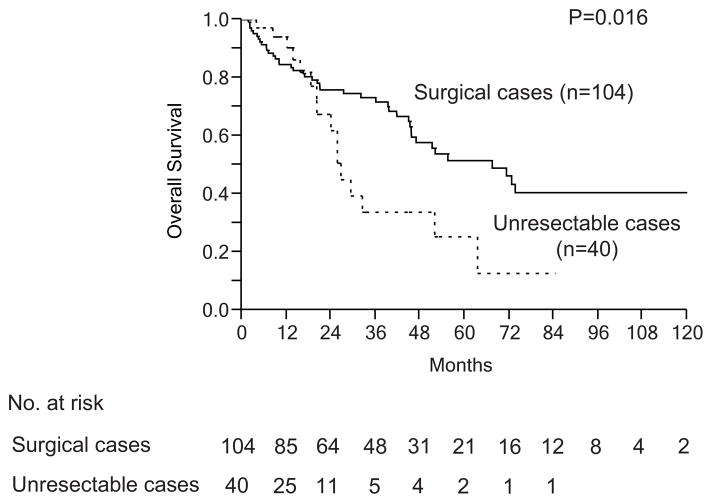
Results: Percutaneous PVE was successfully performed in 141 of the 144 study patients (97.9%). Adequate regeneration was observed in 139 patients (98.5%) with median post-PVE LR/BW rising from 0.33% to 0.52% (p < 0.0001), representing a per-patient median regeneration rate of 62% (range 0.3% to 379%). In total, 104 patients underwent extended right hepatectomy (n = 102) or right hepatectomy (n = 2). The remaining 40 patients (27.8%) were not resectable due to short-interval disease progression (27 patients, 18.5%), insufficient liver regeneration (5 patients, 3.5%), and medical comorbidities (8 patients, 5.6%). After resection, the following outcomes were observed: major morbidity: 33.0% (34 of 104), liver insufficiency: 12.5% (13 of 104), and 90-day liver-related mortality: 5.8% (6 of 104). These oncologic and technical results compare favorably with those of ALPPS.
Conclusions: Based on its ability to select oncologically resectable patients and superior safety and efficacy profiles, percutaneous right + segment IV PVE and interval surgery remains the standard of care for patients with very low future liver remnant volumes.
Copyright © 2013 American College of Surgeons. Published by Elsevier Inc. All rights reserved.
Figures

References
-
- Bax HR, Mansens BJ, Schalm L. Atrophy of the liver after occlusion of the bile ducts or portal vein and compensatory hypertrophy of the unoccluded portion and its clinical importance. Gastroenterology. 1956 Aug;31(2):131–155. - PubMed
-
- Honjo I, Suzuki T, Ozawa K, Takasan H, Kitamura O. Ligation of a branch of the portal vein for carcinoma of the liver. American journal of surgery. 1975 Sep;130(3):296–302. - PubMed
-
- Takayasu K, Muramatsu Y, Shima Y, Moriyama N, Yamada T, Makuuchi M. Hepatic lobar atrophy following obstruction of the ipsilateral portal vein from hilar cholangiocarcinoma. Radiology. 1986 Aug;160(2):389–393. - PubMed
-
- Madoff DC, Abdalla EK, Gupta S, et al. Transhepatic ipsilateral right portal vein embolization extended to segment IV: improving hypertrophy and resection outcomes with spherical particles and coils. J Vasc Interv Radiol. 2005 Feb;16(2 Pt 1):215–225. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
