

Fingolimod versus intramuscular interferon in patient subgroups from TRANSFORMS
- PMID: 23632946
- PMCID: PMC3737385
- DOI: 10.1007/s00415-013-6932-0
Fingolimod versus intramuscular interferon in patient subgroups from TRANSFORMS
Abstract
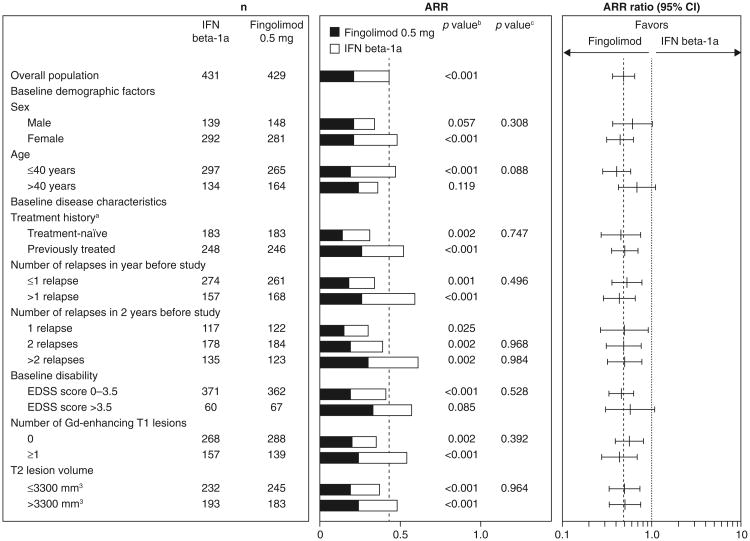
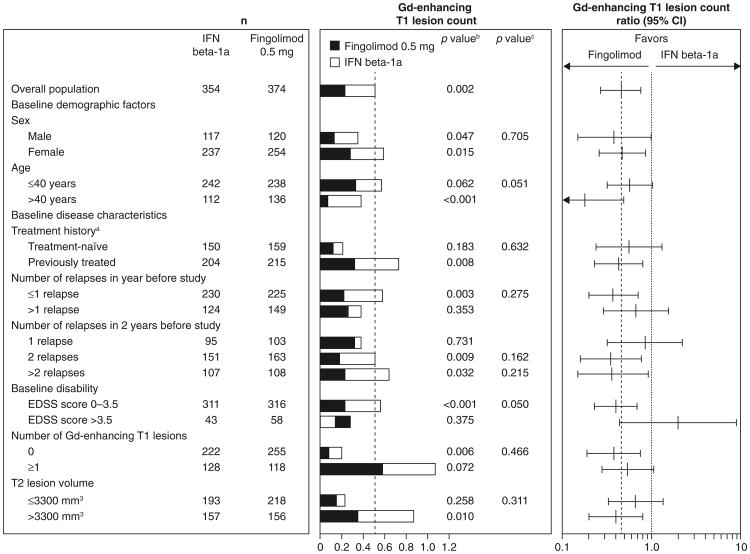
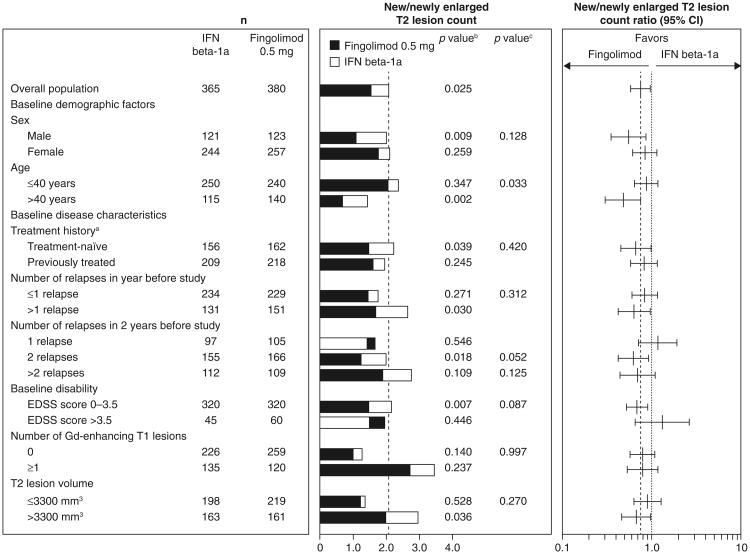
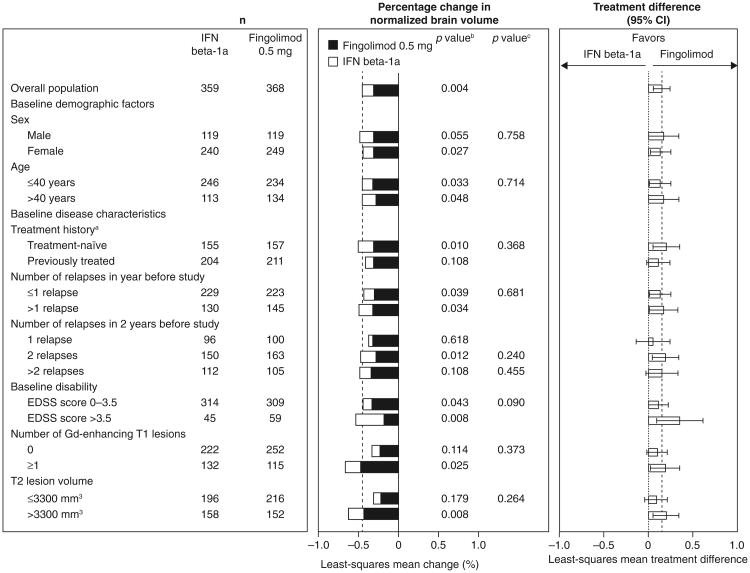
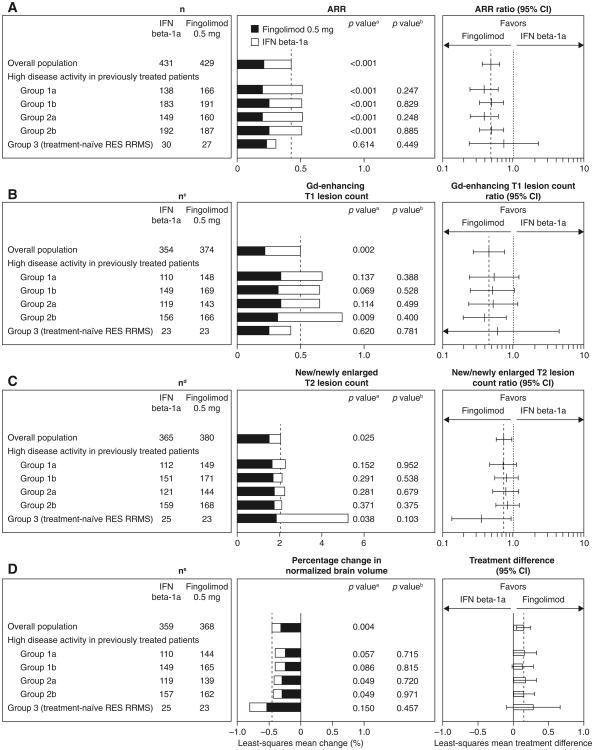
In the 12-month phase 3 TRANSFORMS study, fingolimod showed greater efficacy than intramuscular interferon beta (IFNβ)-1a in patients with relapsing-remitting multiple sclerosis (RRMS). This study analyzed fingolimod efficacy compared with IFNβ-1a in patient subgroups from TRANSFORMS. Patients were randomized to receive fingolimod or weekly IM IFNβ-1a for 12 months. Analyses of efficacy included annualized relapse rate (ARR), and magnetic resonance imaging (MRI) measures [gadolinium (Gd)-enhancing T1 lesions, new/newly enlarged (active) T2 lesions, brain volume change]. Subgroups were defined based on demographics, disease characteristics (baseline EDSS score, relapse rate, and MRI parameters), and response to previous therapy. Fingolimod 0.5 mg reduced ARR over 12 months by 32-59 % relative to IFNβ-1a in all subgroups defined by demographic factors or baseline disease characteristics. Fingolimod also reduced the number of new Gd-enhancing lesions, active T2 lesions, and the rate of brain volume loss, versus IFNβ-1a in most (95 %) subgroups. In patients with high disease activity despite IFNβ treatment in the year before study, fingolimod 0.5 mg reduced ARR by 61 % relative to IFNβ-1a. Reductions in lesion counts and brain volume loss also favored fingolimod in these patients. In conclusion, consistently better efficacy was observed for fingolimod compared with IFNβ-1a across different subgroups of patients with RRMS.
Conflict of interest statement
Figures
References
-
- Cohen JA, Barkhof F, Comi G, Hartung HP, Khatri BO, Montalban X, Pelletier J, Capra R, Gallo P, Izquierdo G, Tiel-Wilck K, de Vera A, Jin J, Stites T, Wu S, Aradhye S, Kappos L. Oral fingolimod or intramuscular interferon for relapsing multiple sclerosis. N Engl J Med. 2010;362:402–415. - PubMed
-
- Kappos L, Radue EW, O'Connor P, Polman C, Hohlfeld R, Calabresi P, Selmaj K, Agoropoulou C, Leyk M, Zhang-Auberson L, Burtin P. A placebo-controlled trial of oral fingolimod in relapsing multiple sclerosis. N Engl J Med. 2010;362(5):387–401. - PubMed
-
- Khatri B, Barkhof F, Comi G, Hartung HP, Kappos L, Montalban X, Pelletier J, Stites T, Wu S, Holdbrook F, Zhang-Auberson L, Francis G, Cohen JA. Comparison of fingolimod with interferon beta-1a in relapsing-remitting multiple sclerosis: a randomised extension of the TRANSFORMS study. Lancet Neurol. 2011;10(6):520–529. - PubMed
-
- Brex PA, Ciccarelli O, O'Riordan JI, Sailer M, Thompson AJ, Miller DH. A longitudinal study of abnormalities on MRI and disability from multiple sclerosis. N Engl J Med. 2002;346(3):158–164. - PubMed
-
- Confavreux C, Vukusic S. Age at disability milestones in multiple sclerosis. Brain. 2006;129(Pt 3):595–605. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
