

Interval debulking surgery for advanced epithelial ovarian cancer
- PMID: 23633332
- PMCID: PMC4161115
- DOI: 10.1002/14651858.CD006014.pub6
Interval debulking surgery for advanced epithelial ovarian cancer
Update in
-
Interval debulking surgery for advanced epithelial ovarian cancer.Cochrane Database Syst Rev. 2016 Jan 9;2016(1):CD006014. doi: 10.1002/14651858.CD006014.pub7. Cochrane Database Syst Rev. 2016. PMID: 26747297 Free PMC article.
Abstract
Background: Interval debulking surgery (IDS), following induction or neoadjuvant chemotherapy, may have a role in treating advanced epithelial ovarian cancer (stage III to IV) where primary debulking surgery is not an option.
Objectives: To assess the effectiveness and complications of IDS for women with advanced stage epithelial ovarian cancer.
Search methods: We searched the Cochrane Gynaecological Cancer Group's Specialised Register to June 2012, the Cochrane Central Register of Controlled Trials (CENTRAL) 2012, Issue 6, MEDLINE to June 2012 and EMBASE to June 2012.
Selection criteria: Randomised controlled trials (RCTs) comparing survival of women with advanced epithelial ovarian cancer, who had IDS performed between cycles of chemotherapy after primary surgery with survival of women who had conventional treatment (primary debulking surgery and adjuvant chemotherapy).
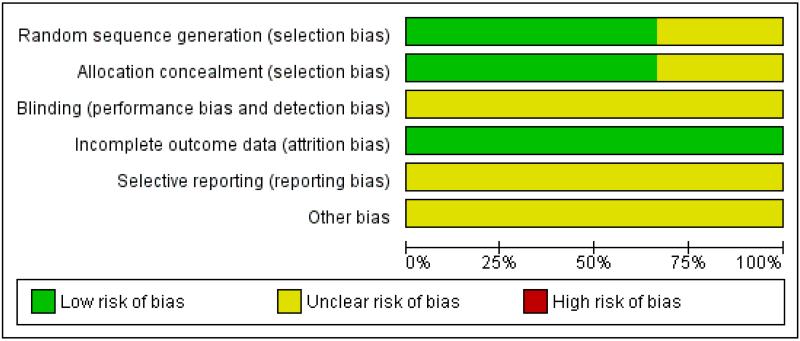
Data collection and analysis: Two review authors independently assessed trial quality and extracted data. Searches for additional information from study authors were attempted. We performed meta-analysis of overall and progression-free survival (PFS), using random-effects models.
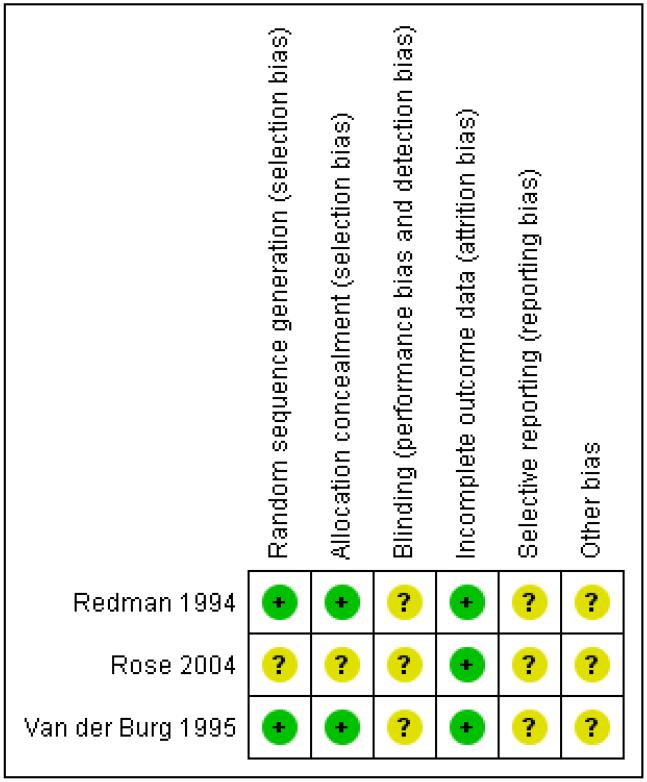
Main results: Three RCTs randomising 853 women, of whom 781 were evaluated, met the inclusion criteria. Meta-analysis of three trials for overall survival (OS) found no statistically significant difference between IDS and chemotherapy alone (hazard ratio (HR) = 0.80, 95% confidence interval (CI) 0.61 to 1.06, I² = 58%). Subgroup analysis for OS in two trials, where the primary surgery was not performed by gynaecologic oncologists or was less extensive, showed a benefit of IDS (HR = 0.68, 95% CI 0.53 to 0.87, I² = 0%). Meta-analysis of two trials for PFS found no statistically significant difference between IDS and chemotherapy alone (HR = 0.88, 95% CI 0.57 to 1.33, I² = 83%). Rates of toxic reactions to chemotherapy were similar in both arms (risk ratio = 1.19, 95% CI 0.53 to 2.66, I² = 0%), but little information was available for other adverse events or quality or life (QoL).
Authors' conclusions: We found no conclusive evidence to determine whether IDS between cycles of chemotherapy would improve or decrease the survival rates of women with advanced ovarian cancer, compared with conventional treatment of primary surgery followed by adjuvant chemotherapy. IDS appeared to yield benefit only in women whose primary surgery was not performed by gynaecologic oncologists or was less extensive. Data on QoL and adverse events were inconclusive.
Figures
Update of
-
Interval debulking surgery for advanced epithelial ovarian cancer.Cochrane Database Syst Rev. 2010 Oct 6;(10):CD006014. doi: 10.1002/14651858.CD006014.pub5. Cochrane Database Syst Rev. 2010. Update in: Cochrane Database Syst Rev. 2013 Apr 30;(4):CD006014. doi: 10.1002/14651858.CD006014.pub6. PMID: 20927744 Updated.
References
References to studies included in this review
-
-
*
- Redman CW, Warwick J, Luesley DM, Varma R, Lawton FG, Blackledge GR. Intervention debulking surgery in advanced epithelial ovarian cancer. British Journal of Obstetrics and Gynaecology. 1994;101:142–6. - PubMed
-
-
- Varma R, Blackledge G, Redman C, Luesley D, Chan KK, Mould J. A randomised trial of intervention debulking surgery and the duration of cis-platinum combination chemotherapy in advanced epithelial ovarian cancer (EOC) Annals of Oncology. 1990;1(Suppl 9):4.
-
- Rose PG, Nerenston S, Brady MF, Clarke Pearson D, Olt G, Rubin SC, et al. Operative morbidity following primary and interval debulking surgery for advanced ovarian cancer. Proceedings of the American Society of Clinical Oncology. 2004;23:450.
-
- Rose PG, Nerenstone S, Brady M, Clarke Pearson D, Olt G, Rubin SC, et al. A phase III randomised study of interval secondary cytoreduction in patients with advanced stage ovarian carcinoma with suboptimal residual disease: a Gynecologic Oncology Group study. Proceedings of the American Society of Clinical Oncology. 2002;21(Pt 1):201a.
-
-
*
- Rose PG, Nerenstone S, Brady MF, Clarke-Pearson D, Olt G, Rubin SC, et al. Secondary surgical cytoreduction for advanced ovarian carcinoma. The New England Journal of Medicine. 2004;351:2489–97. - PubMed
-
References to studies excluded from this review
-
- Angioli R, Palaia I, Zullo MA, Muzii L, Manci N, Calcagno M, et al. Diagnostic open laparoscopy in the management of advanced ovarian cancer. Gynecologic Oncology. 2006;100:455–61. - PubMed
-
- Chan YM, Ng TY, Ngan HY, Wong LC. Quality of life in women treated with neoadjuvant chemotherapy for advanced ovarian cancer: a prospective longitudinal study. Gynecologic Oncology. 2003;88:9–16. - PubMed
-
- Dutta T, Sharma H, Kumar L, Dinda AK, Kumar S, Bhatla N, et al. Neoadjuvant chemotherapy for epithelial ovarian cancer--role of apoptosis. Cancer Chemotherapy and Pharmacology. 2005;56(4):427–35. - PubMed
-
- Evdokimova NI, Grigorova TM. Comparative study of 2 combined treatment regimens in stage-III to -IV ovarian cancer. Voprosy onkologii. 1982;28(7):28–34. - PubMed
-
- Fuso L, Amant F, Neven P, Berteloot P, Vergote I. Gemcitabine-carboplatin-paclitaxel combination as first-line therapy in advanced ovarian carcinoma: A single institution phase II study in 24 patients. International Journal of Gynecological Cancer. 2006;16(Suppl 1):60–7. - PubMed
Additional references
-
- Ansquer Y, Leblanc E, Clough K, Morice P, Dauplat J, Mathevet P, et al. Neoadjuvant chemotherapy for unresectable ovarian carcinoma. Cancer. 2001;91:2329–34. - PubMed
-
- Bristow RE, Tomacruz RS, Armstrong DK, Trimble EL, Montz FJ. Survival effect of maximal cytoreductive surgery for advanced ovarian carcinoma during the platinum era: a meta-analysis. Journal of Clinical Oncology. 2002;20:1248–59. - PubMed
-
- Bristow RE, Chi DS. Platinum-based neoadjuvant chemotherapy and interval surgical cytoreduction for advanced ovarian cancer: a meta-analysis. Gynecologic Oncology. 2006;103(3):1070–6. - PubMed
-
- Bristow RE, Eisenhauer EL, Santillan A, Chi DS. Delaying the primary surgical effort for advanced ovarian cancer: a systematic review of neoadjuvant chemotherapy and interval cytoreduction. Gynecologic Oncology. 2007;104(2):480–90. - PubMed
-
- Bucher HC, Guyatt GH, Griffith LE, Walter SD. The results of direct and indirect treatment comparisons in meta-analysis of randomized controlled trials. Journal of Clinical Epidemiology. 1997;50(6):683–91. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous