

Differentiating nonrestorative sleep from nocturnal insomnia symptoms: demographic, clinical, inflammatory, and functional correlates
- PMID: 23633749
- PMCID: PMC3624821
- DOI: 10.5665/sleep.2624
Differentiating nonrestorative sleep from nocturnal insomnia symptoms: demographic, clinical, inflammatory, and functional correlates
Abstract
Study objectives: Recent studies have suggested that nonrestorative sleep (NRS) symptoms may be distinct from nocturnal insomnia symptoms (NIS). However, there is limited information on the demographic, medical, and biologic correlates of NRS independent from NIS in the general population. This report presents the sociodemographic correlates, patterns of comorbidity with other sleep and physical disorders, C-reactive protein (CRP) levels, and general productivity associated with NIS and NRS in a nationally representative sample of US adults.
Design: National Health and Nutrition Examination Survey (NHANES).
Setting: The 2005-2008 surveys of the general population in the United States.
Participants: There were 10,908 individuals (20 years or older).
Interventions: N/A.
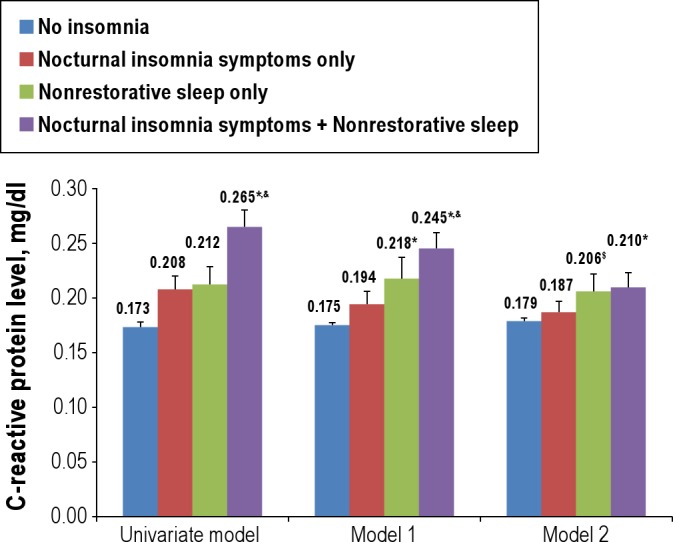
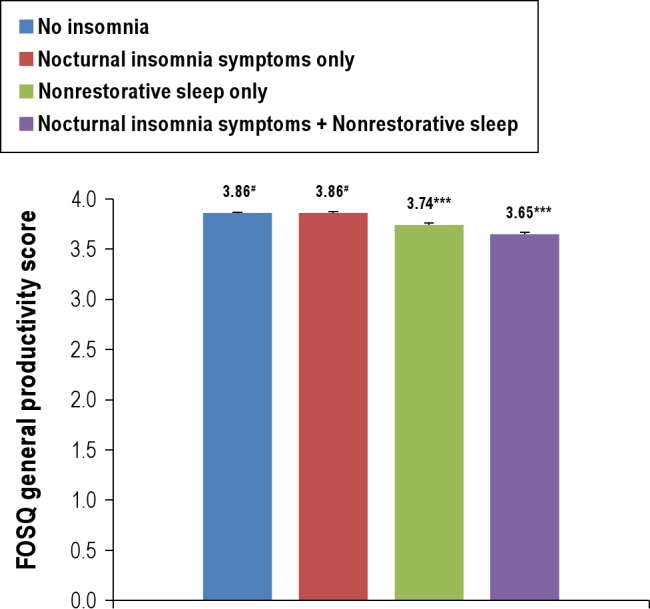
Measurements and results: Respondents were classified by the presence or absence of NIS and NRS. Compared with those without insomnia symptoms, respondents with NIS were older and had lower family income and educational levels than those with NRS. In addition, there was a significant association between NIS and cardiovascular disease, whereas NRS was associated with other primary sleep disorders (including habitual snoring, sleep apnea, and restless legs syndrome), respiratory diseases (emphysema and chronic bronchitis), thyroid disease, and cancer as well as increased CRP levels. In addition, the study participants with NRS only reported poorer scores on the Functional Outcomes of Sleep Questionnaire (FOSQ) than those without insomnia symptoms or those with NIS only.
Conclusions: These findings suggest that there are substantial differences between NIS and NRS in terms of sociodemographic factors, comorbidity with other sleep and physical disorders, increased CRP level, and functional impairment. An inflammatory response might play a unique role in the pathogenesis of NRS.
Keywords: C-reactive protein; functional impairment; medical condition; nocturnal insomnia symptoms; nonrestorative sleep..
Figures
Comment in
-
Nonrestorative sleep: a new perspective.Sleep. 2013 May 1;36(5):633-4. doi: 10.5665/sleep.2612. Sleep. 2013. PMID: 23633743 Free PMC article. No abstract available.
References
-
- Pearson NJ, Johnson LL, Nahin RL. Insomnia, trouble sleeping, and complementary and alternative medicine: analysis of the 2002 national health interview survey data. Arch Intern Med. 2006;166:1775–82. - PubMed
-
- Mellinger GD, Balter MB, Uhlenhuth EH. Insomnia and its treatment. Prevalence and correlates. Arch Gen Psychiatry. 1985;42:225–32. - PubMed
-
- Roth T, Coulouvrat C, Hajak G, et al. Prevalence and perceived health associated with insomnia based on DSM-IV-TR; International Statistical Classification of Diseases and Related Health Problems, Tenth Revision; and Research Diagnostic Criteria/International Classification of Sleep Disorders, Second Edition criteria: results from the America Insomnia Survey. Biol Psychiatry. 2011;69:592–600. - PubMed
-
- American Academy of Sleep Medicine. International classification of sleep disorders: diagnostic and coding manual. 2nd ed. Westchester, IL: American Academy of Sleep Medicine; 2005.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
