

Sensitization of upper airway mechanoreceptors as a new pharmacologic principle to treat obstructive sleep apnea: investigations with AVE0118 in anesthetized pigs
- PMID: 23633752
- PMCID: PMC3624824
- DOI: 10.5665/sleep.2630
Sensitization of upper airway mechanoreceptors as a new pharmacologic principle to treat obstructive sleep apnea: investigations with AVE0118 in anesthetized pigs
Abstract
Study objectives: Drug treatment for obstructive sleep apnea (OSA) is desirable because at least 30% of patients do not tolerate continuous positive airway pressure (CPAP) treatment. The negative pressure reflex (NPR) involving superficially located mechanoreceptors in the upper airway (UA) is an important mechanism for UA patency inhibitable by topical UA anesthesia (lidocaine). The NPR may serve as a target for pharmacological intervention for a topical treatment of OSA. The objective was to determine the effect of pharmacological augmentation of the NPR on UA collapsibility.
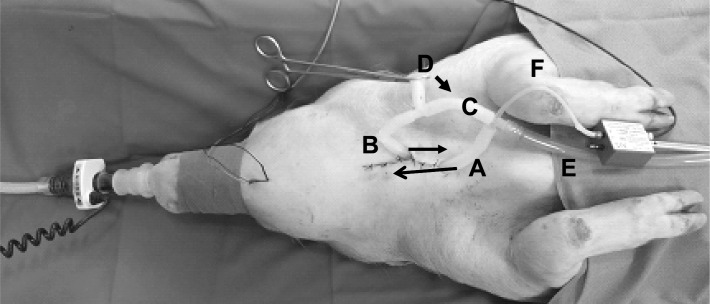
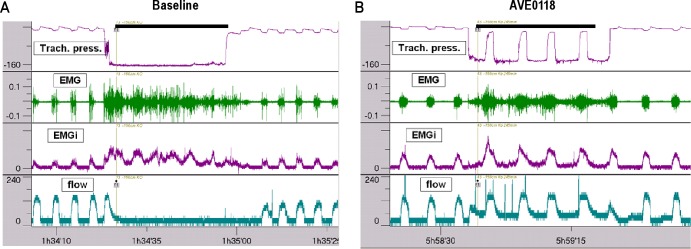
Design: We developed a model of UA collapsibility in which application of negative pressures caused UA collapses in spontaneously breathing α-chloralose-urethane anesthetized pigs as indicated by characteristic tracheal pressure and air flow changes.
Setting: N/A.
Patients or participants: N/A.
Interventions: N/A.
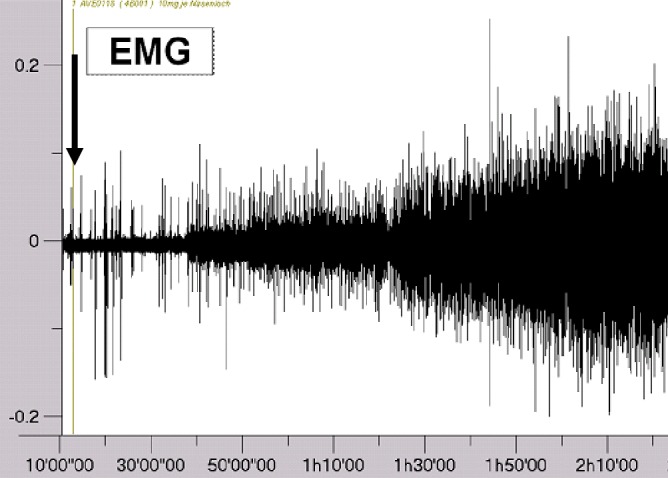
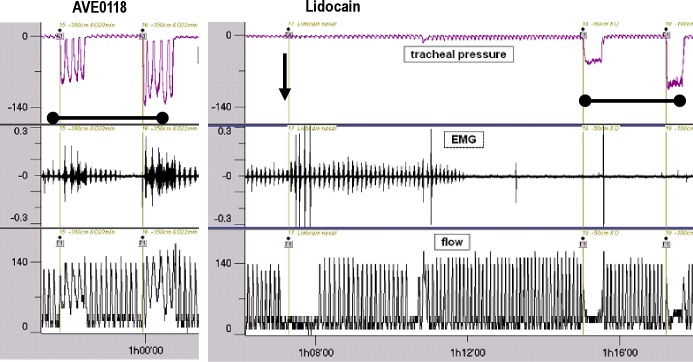
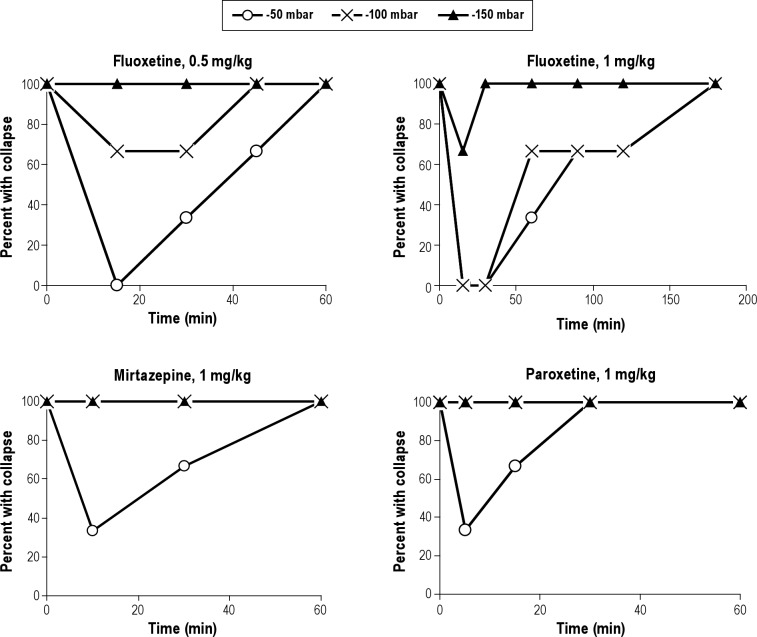
Measurements and results: The potassium channel blocker AVE0118 administered topically to the UA in doses of 1, 3, and 10 mg per nostril sensitized the NPR, shifting the mechanoreceptor response threshold for the genioglossus muscle to more positive pressures (P < 0.001; n = 6 per group) and dose-dependently inhibited UA collapsibility. Ten mg of AVE0118 prevented UA collapses against negative pressures of -150 mbar (P < 0.01) for > 4 h in all pigs, while in control pigs the UA collapsed at -50 mbar or less negative pressures. The effect of AVE0118 was abolished by UA lidocaine anesthesia. Acute intravenous administration of naloxone or acetazolamide was ineffective; paroxetine and mirtazepine were weakly effective and fluoxetine was moderately effective in line with reported clinical efficacy.
Conclusion: Topical administration of AVE0118 to the UA is a promising pharmacologic approach for the treatment of OSA.
Keywords: AVE0118; Animal model; mechanoreceptors; negative pressure reflex; obstructive sleep apnea.
Figures

Comment in
-
A new pharmacological treatment to treat obstructive sleep apnea?Sleep. 2013 May 1;36(5):635-6. doi: 10.5665/sleep.2614. Sleep. 2013. PMID: 23633744 Free PMC article. No abstract available.
References
-
- Young T, Peppard PE, Gottlieb DJ. Epidemiology of obstructive sleep apnea: a population health perspective. Am J Respir Crit Care Med. 2002;165:1217–39. - PubMed
-
- Resnick HE, Redline S, Shahar E, et al. Diabetes and sleep disturbances: findings from the Sleep Heart Health Study. Diabetes Care. 2003;26:702–9. - PubMed
-
- Baguet JP, Barone-Rochette G, Pepin JL. Hypertension and obstructive sleep apnoea syndrome: current perspectives. J Hum Hypertens. 2009;23:431–43. - PubMed
-
- Kohler M, Smith D, Tippett V, Stradling JR. Predictors of long-term compliance with continuous positive airway pressure. Thorax. 2010;65:829–32. - PubMed
-
- Hedner J, Grote L, Zou D. Pharmacological treatment of sleep apnea: current situation and future strategies. Sleep Med Rev. 2008;12:33–47. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
