

Treacher collins syndrome
- PMID: 23633935
- PMCID: PMC3424693
- DOI: 10.1055/s-0032-1320066
Treacher collins syndrome
Abstract
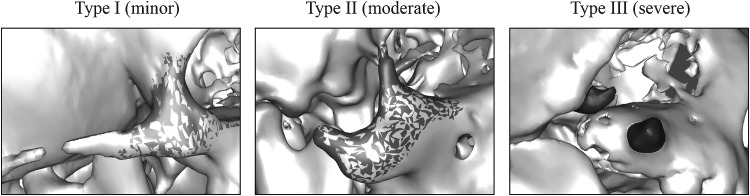
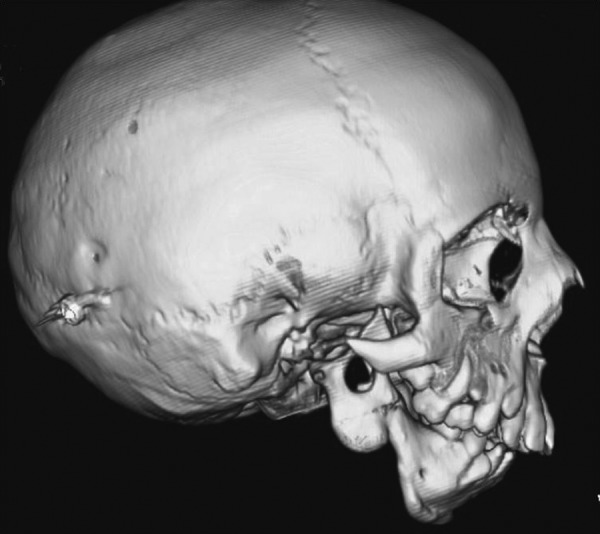
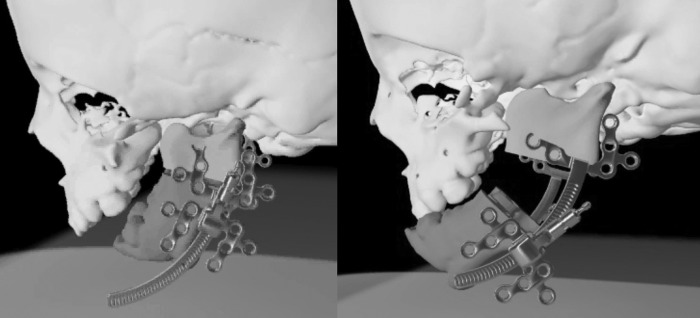
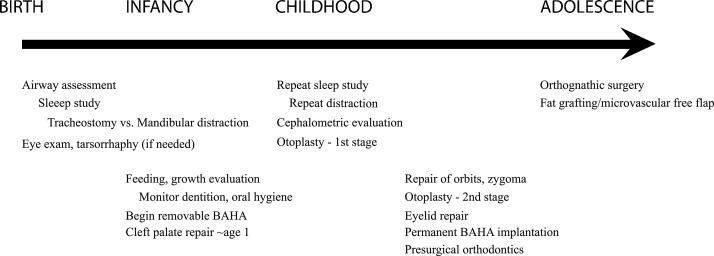
Treacher Collins syndrome is a genetic disorder resulting in congenital craniofacial malformation. Patients typically present with downslanting palpebral fissures, lower eyelid colobomas, microtia, and malar and mandibular hypoplasia. This autosomal dominant disorder has a variable degree of phenotypic expression, and patients have no associated developmental delay or neurologic disease. Care for these patients requires a multidisciplinary team from birth through adulthood. Proper planning, counseling and surgical techniques are essential for optimizing patient outcomes. Here the authors review the features, genetics, and treatment of Treacher Collins syndrome.
Keywords: Franceschetti-Klein syndrome; Treacher Collins syndrome; facial clefting; malar hypoplasia; mandibular distraction; mandibulofacial dysostosis; microsomia; microtia.
Figures



References
-
- Scully C, Langdon J, Evans J. Marathon of eponyms: 20 Treacher Collins syndrome. Oral Dis. 2011;17(6):619–620. - PubMed
-
- Collins E T. Cases with symmetrical congenital notches in the outer part of each lid and defective development of the malar bones. Trans Ophthalmol Soc U K. 1900;20:190–192.
-
- Franceschetti A, Klein D. The mandibulofacial dysostosis; a new hereditary syndrome. Acta Ophthalmol (Copenh) 1949;27(2):143–224. - PubMed
-
- Dixon J, Trainor P, Dixon M J. Treacher Collins syndrome. Orthod Craniofac Res. 2007;10(2):88–95. - PubMed
