

Microbial dysbiosis and colon carcinogenesis: could colon cancer be considered a bacteria-related disease?
- PMID: 23634186
- PMCID: PMC3625019
- DOI: 10.1177/1756283X12473674
Microbial dysbiosis and colon carcinogenesis: could colon cancer be considered a bacteria-related disease?
Abstract
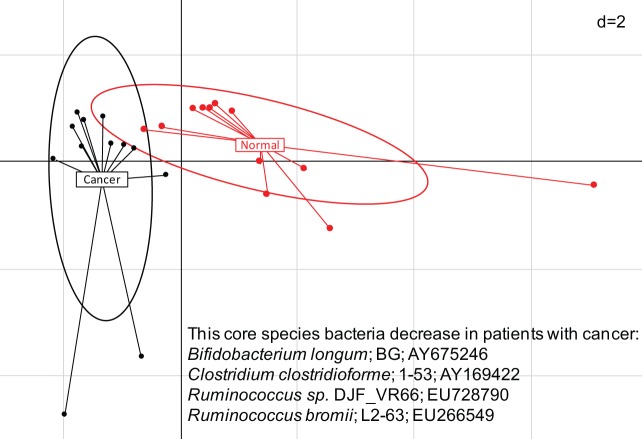
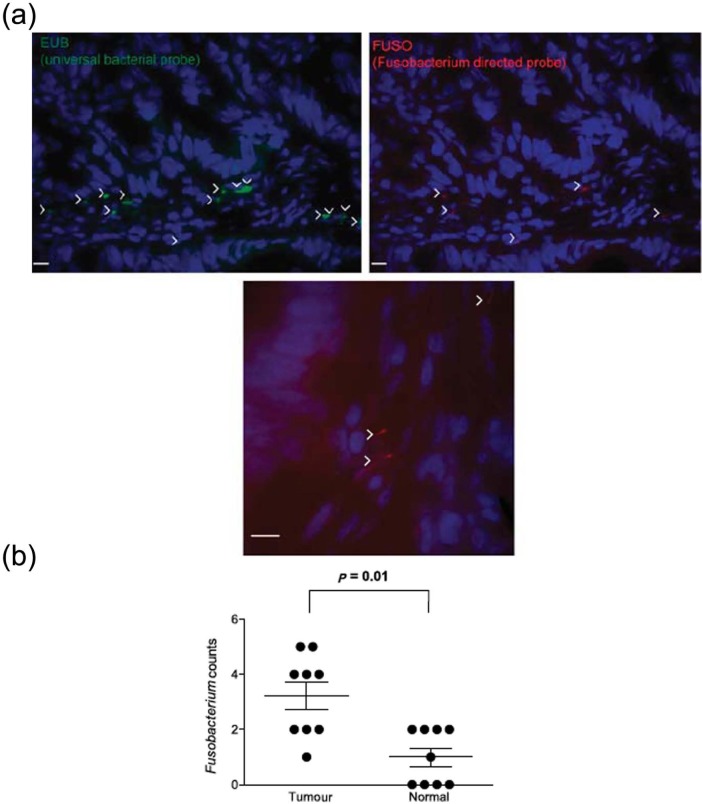
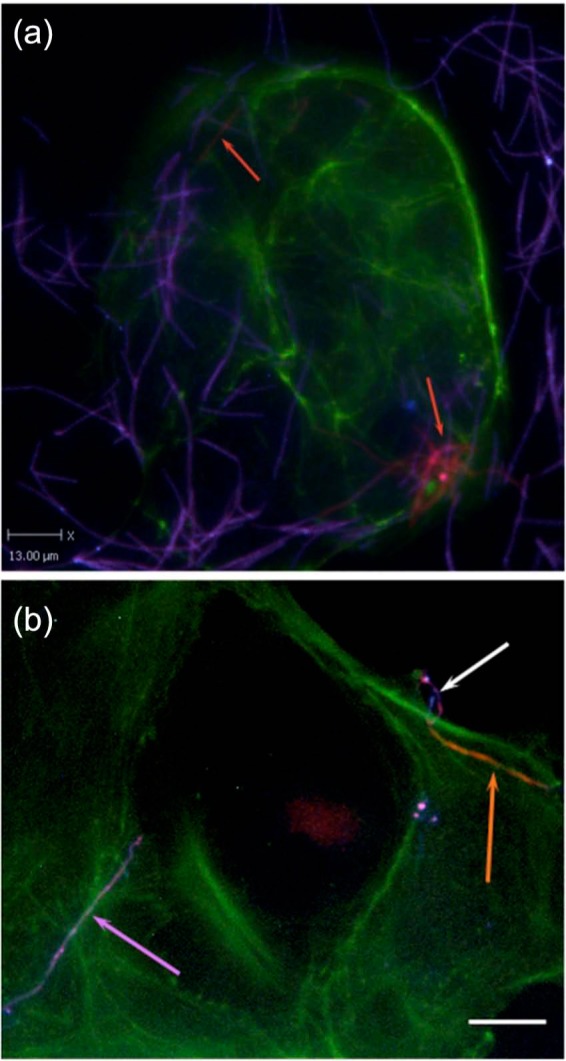
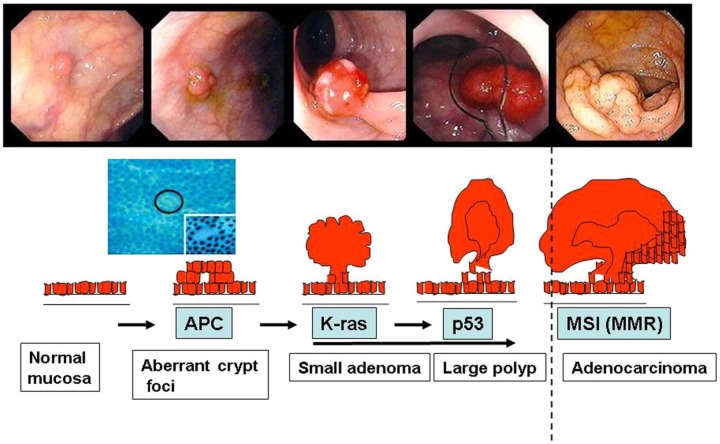
Colorectal cancer (CRC) is posing an increasingly important burden on the health care system, with western countries seeing a growing incidence of the disease. Except for germline DNA mutations which have been attributed to less than 5% of patients, little is known about the main causes of CRC. However, environment factors such as food, lifestyle and medication are now suspected to have a major influence on inducing cancers. Today, exhaustive quantitative and qualitative evaluation of all environmental factors is not possible. Various environment-induced diseases have been characterized based on colon microflora, also called microbiota, analyses. Growing data have shown specific changes in microflora (i.e. dysbiosis) in the stools of patients with colon cancer or those adherent to the colonic mucosa. Thus, it appears that microbiota may be considered a platform offering host and environment interactions for studying CRCs. The hypothesis that colon cancer might be a bacteria-related disease is suggested and perspectives are discussed.
Keywords: bacteria; bacteria–host interaction; colon cancer; environment; genetic.
Conflict of interest statement
Figures
References
-
- Aparicio T., Kermorgant S., Darmoul D., Guilmeau S., Hormi K., Mahieu-Caputo D., et al. (2005) Leptin and Ob-Rb receptor isoform in the human digestive tract during fetal development. J Clin Endocrinol Metab 90: 6177–6184 - PubMed
-
- Bach J. (2002) The effect of infections on susceptibility to autoimmune and allergic diseases. N Engl J Med 347: 911–920 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
