

Immunotherapeutic approaches in triple-negative breast cancer: latest research and clinical prospects
- PMID: 23634195
- PMCID: PMC3630481
- DOI: 10.1177/1758834012475152
Immunotherapeutic approaches in triple-negative breast cancer: latest research and clinical prospects
Abstract
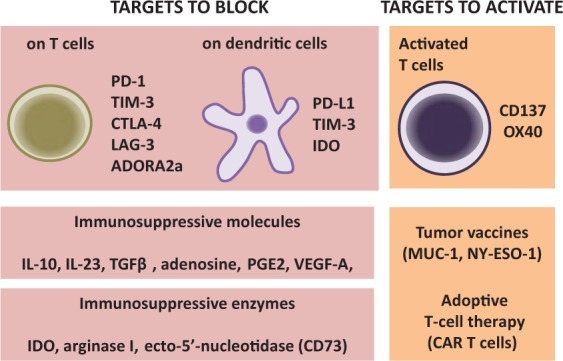
Triple-negative breast cancer (TNBC), as defined by the absence of estrogen receptor, progesterone receptor and human epidermal growth factor receptor 2 expression, is a challenging disease with the poorest prognosis of all breast cancer subtypes. Importantly, there are currently no known molecular targets for this subgroup of patients. Recent advances in genomics and gene expression profiling have shed new light on the molecule heterogeneity of TNBC. We present an overview of the scientific evidence suggesting that clinical outcome in TNBC is affected by tumor-infiltrating immune cells. We also describe tumor-associated antigens recently identified in TNBC. Finally, we review the current literature on promising immunotherapies for TNBC, including tumor vaccine approaches, immune-checkpoint inhibitors, antagonists of immunosuppressive molecules and adoptive cell therapies. It is our contention that selected patients with TNBC with lymphocytic tumor infiltrates at diagnosis may benefit from immune-based therapies and that these immunotherapies will be most beneficial in combination with cytotoxic drugs that potentiate adaptive anti-tumor immunity.
Keywords: T cell; basal like; breast cancer; immunotherapy.
Conflict of interest statement
Figures
References
-
- Arnes J., Brunet J., Stefansson I., Bégin L., Wong N., Chappuis P., et al. (2005) Placental cadherin and the basal epithelial phenotype of BRCA1-related breast cancer. Clin Cancer Res 11: 4003–4011 - PubMed
-
- Bauer K., Brown M., Cress R., Parise C., Caggiano V. (2007) Descriptive analysis of estrogen receptor (ER)-negative, progesterone receptor (PR)-negative, and HER2-negative invasive breast cancer, the so-called triple-negative phenotype. Cancer 109: 1721–1728 - PubMed
-
- Bertucci F., Finetti P., Cervera N., Charafe-Jauffret E., Mamessier E., Adélaïde J., et al. (2006) Gene expression profiling shows medullary breast cancer is a subgroup of basal breast cancers. Cancer Res 66: 4636–4644 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
