

The evaluation of a patient with dizziness
- PMID: 23634356
- PMCID: PMC3613190
- DOI: 10.1212/CPJ.0b013e31823d07b6
The evaluation of a patient with dizziness
Abstract
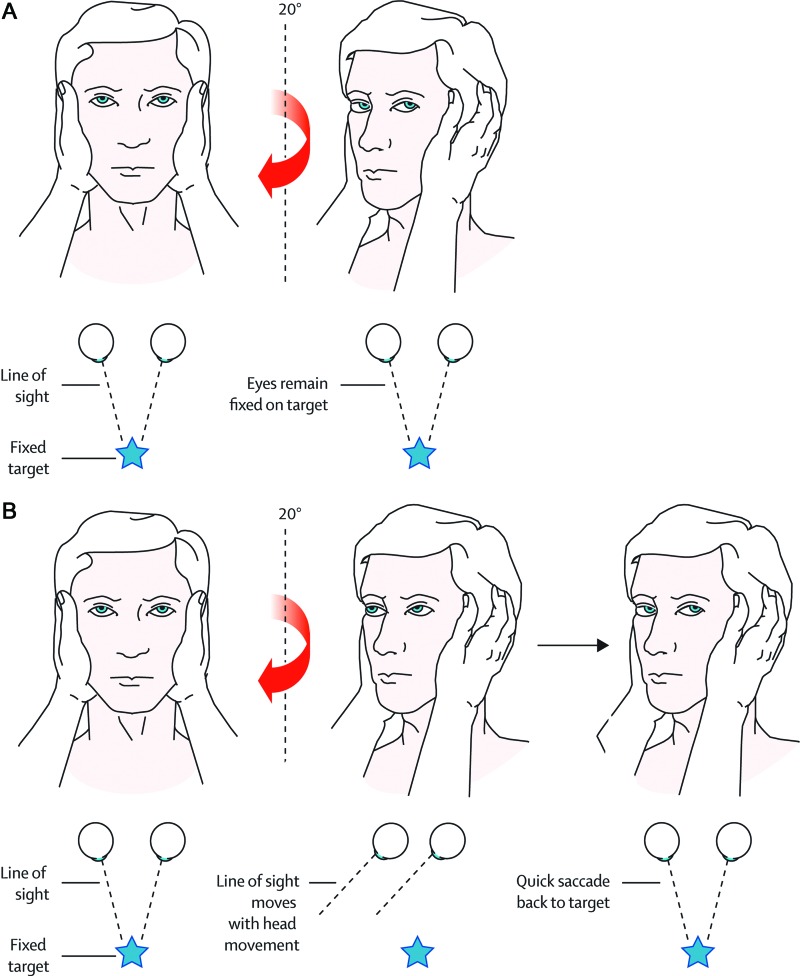
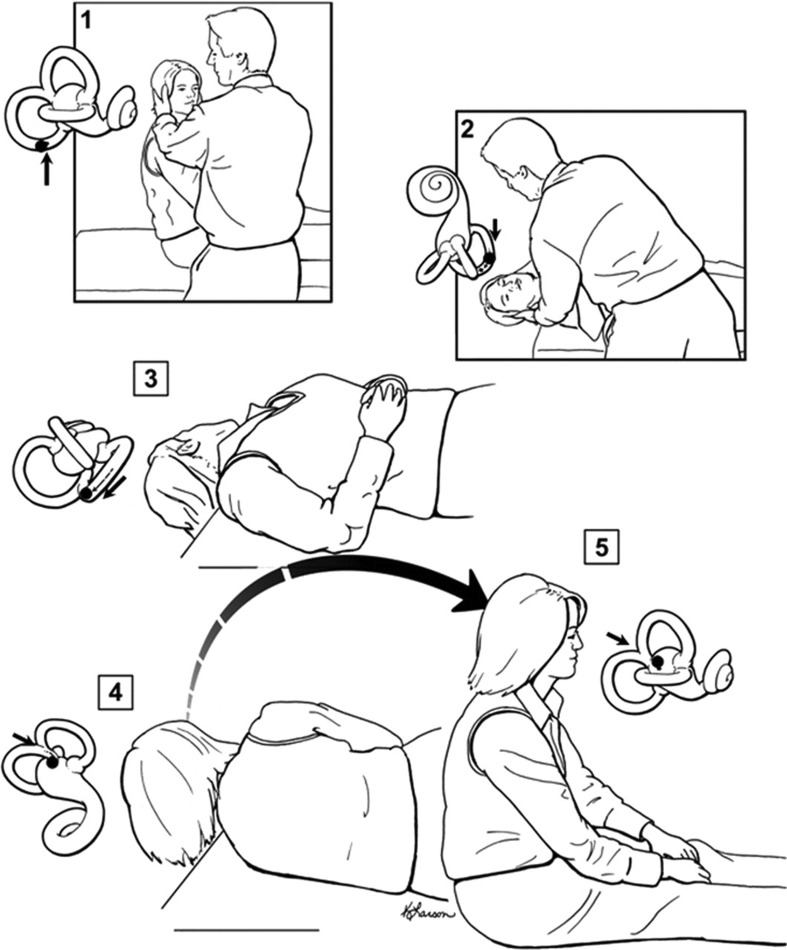
Dizziness is the quintessential symptom presentation in all of clinical medicine. It can stem from a disturbance in nearly any system of the body. Patient descriptions of the symptom are often vague and inconsistent, so careful probing is essential. The physical examination is performed by observing the patient at rest and following simple movements or bedside tests. In general, no special tools are required. The causes of dizziness range from benign to life-threatening disorders, and features that distinguish among these may be subtle. When diagnostic testing is considered, parsimony should be the rule. Identifying common peripheral vestibular disorders is a priority. Picking this "low hanging fruit" can be the key component to excluding more serious central causes of dizziness.
Figures
References
-
- Eagles D, Stiell IG, Clement CM, et al. International survey of emergency physicians' priorities for clinical decision rules. Acad Emerg Med 2008;15:177–182 - PubMed
-
- Newman-Toker DE, Cannon LM, Stofferahn ME, Rothman RE, Hsieh YH, Zee DS. Imprecision in patient reports of dizziness symptom quality: a cross-sectional study conducted in an acute care setting. Mayo Clin Proc 2007;82:1329–1340 - PubMed
-
- Neuhauser H, Lempert T. Vestibular migraine. Neurol Clin 2009;27:379–391 - PubMed
LinkOut - more resources
Full Text Sources
Medical