

World society of emergency surgery study group initiative on Timing of Acute Care Surgery classification (TACS)
- PMID: 23634784
- PMCID: PMC3652724
- DOI: 10.1186/1749-7922-8-17
World society of emergency surgery study group initiative on Timing of Acute Care Surgery classification (TACS)
Abstract
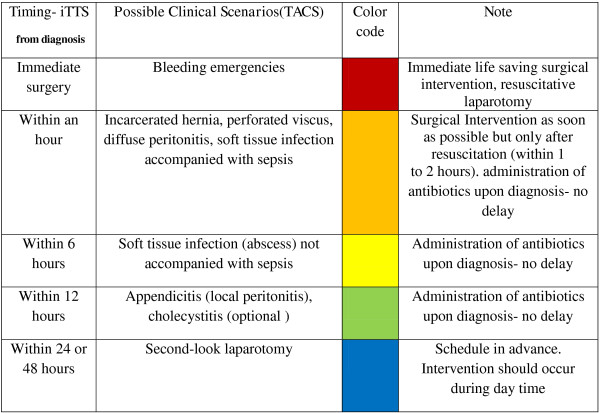
Timing of surgical intervention is critical for outcomes of patients diagnosed with surgical emergencies. Facing the challenge of multiple patients requiring emergency surgery, or of limited resource availability, the acute care surgeon must triage patients according to their disease process and physiological state. Emergency operations from all surgical disciplines should be scheduled by an agreed time frame that is based on accumulated data of outcomes related to time elapsed from diagnosis to surgery. Although literature exists regarding the optimal timing of various surgical interventions, implementation of protocols for triage of surgical emergencies is lacking. For institutions of a repetitive triage mechanism, further discussion on optimal timing of surgery in diverse surgical emergencies should be encouraged. Standardizing timing of interventions in surgical emergencies will promote clinical investigation as well as a commitment by administrative authorities to proper operating theater provision for acute care surgery.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
