

Human Papillomavirus-associated oropharyngeal cancer: an observational study of diagnosis, prevalence and prognosis in a UK population
- PMID: 23634887
- PMCID: PMC3644265
- DOI: 10.1186/1471-2407-13-220
Human Papillomavirus-associated oropharyngeal cancer: an observational study of diagnosis, prevalence and prognosis in a UK population
Abstract
Background: The incidence of Human Papillomavirus (HPV) associated oropharyngeal cancer (OPC) is increasing. HPV-associated OPC appear to have better prognosis than HPV-negative OPC. The aim of this study was to robustly determine the prevalence of HPV-positive OPC in an unselected UK population and correlate HPV positivity with clinical outcome.
Methods: HPV testing by GP5+/6+ PCR, In Situ Hybridisation (ISH) and p16 immunohistochemistry (IHC) was performed on 138 OPCs diagnosed in South Wales (UK) between 2001-06. Kaplan-Meier analysis was used to correlate HPV status with clinical outcome.
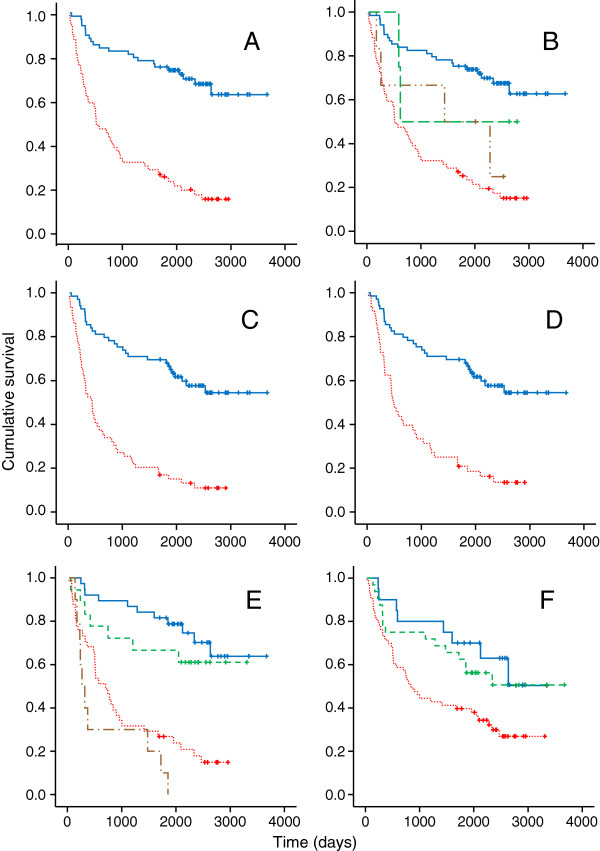
Results: Using a composite definition of HPV positivity (HPV DNA and p16 overexpression), HPV was detected in 46/83 (55%) samples where DNA quality was assured. Five year overall survival was 75.4% (95% CI: 65.2 to 85.5) in HPV-positives vs 25.3% (95% CI: 14.2 to 36.4) in HPV negatives, corresponding to a 78% reduction in death rate (HR 0.22, p < 0.001). HPV-positives had less locoregional recurrence but second HPV-positive Head and Neck primaries occurred. Poor quality DNA in fixed pathological specimens reduced both HPV prevalence estimates and the prognostic utility of DNA-based HPV testing methods. As a single marker, p16 was least affected by sample quality and correlated well with prognosis, although was not sufficient on its own for accurate HPV prevalence reporting.
Conclusions: This study highlights the significant burden of OPC associated with HPV infection. HPV positive cases are clinically distinct from other OPC, and are associated with significantly better clinical outcomes. A composite definition of HPV positivity should be used for accurate prevalence reporting and up-front DNA quality assessment is recommended for any DNA-based HPV detection strategy.
Figures
Similar articles
-
Salivary High-Risk Human Papillomavirus (HPV) DNA as a Biomarker for HPV-Driven Head and Neck Cancers.J Mol Diagn. 2021 Oct;23(10):1334-1342. doi: 10.1016/j.jmoldx.2021.07.005. Epub 2021 Jul 27. J Mol Diagn. 2021. PMID: 34325059 Free PMC article.
-
Study of the concordance between p16 immunohistochemistry and HPV-PCR genotyping for the viral diagnosis of oropharyngeal squamous cell carcinoma.Eur Ann Otorhinolaryngol Head Neck Dis. 2015 Jun;132(3):135-9. doi: 10.1016/j.anorl.2015.01.003. Epub 2015 Feb 14. Eur Ann Otorhinolaryngol Head Neck Dis. 2015. PMID: 25687724
-
The changing incidence of human papillomavirus-associated oropharyngeal cancer using multiple imputation from 2000 to 2010 at a Comprehensive Cancer Centre.Cancer Epidemiol. 2013 Dec;37(6):820-9. doi: 10.1016/j.canep.2013.09.011. Epub 2013 Nov 1. Cancer Epidemiol. 2013. PMID: 24184275
-
HPV-positive head and neck tumours, a distinct clinical entity.B-ENT. 2015;11(2):81-7. B-ENT. 2015. PMID: 26563006 Review.
-
Attributes of HPV associated cancers.Clin Transl Oncol. 2025 Jun 1. doi: 10.1007/s12094-025-03959-1. Online ahead of print. Clin Transl Oncol. 2025. PMID: 40452000 Review.
Cited by
-
Circulating HPV DNA in the Management of Oropharyngeal and Cervical Cancers: Current Knowledge and Future Perspectives.J Clin Med. 2021 Apr 6;10(7):1525. doi: 10.3390/jcm10071525. J Clin Med. 2021. PMID: 33917435 Free PMC article. Review.
-
Human papillomavirus (HPV) and its vaccine: awareness and opinions of clinical dental students in a UK dental school.Br Dent J. 2018 Nov 23;225(10):976-981. doi: 10.1038/sj.bdj.2018.1024. Br Dent J. 2018. PMID: 30468167
-
Geographic variation in human papillomavirus-related oropharyngeal cancer: Data from 4 multinational randomized trials.Head Neck. 2016 Apr;38 Suppl 1(Suppl 1):E1863-9. doi: 10.1002/hed.24336. Epub 2016 Jan 8. Head Neck. 2016. PMID: 26749143 Free PMC article.
-
Mutation analysis of genes in the EGFR pathway in Head and Neck cancer patients: implications for anti-EGFR treatment response.BMC Res Notes. 2014 Jun 4;7:337. doi: 10.1186/1756-0500-7-337. BMC Res Notes. 2014. PMID: 24899223 Free PMC article.
-
The prevalence of human papillomavirus in oropharyngeal cancer in a New Zealand population.PLoS One. 2017 Oct 19;12(10):e0186424. doi: 10.1371/journal.pone.0186424. eCollection 2017. PLoS One. 2017. PMID: 29049330 Free PMC article.
References
-
- Nasman A, Attner P, Hammarstedt L, Du J, Eriksson M, Giraud G, Ahrlund-Richter S, Marklund L, Romanitan M, Lindquist D. Incidence of human papillomavirus (HPV) positive tonsillar carcinoma in Stockholm, Sweden: an epidemic of viral-induced carcinoma? Int J Cancer. 2009;125(2):362–366. doi: 10.1002/ijc.24339. - DOI - PubMed
-
- Hong AM, Dobbins TA, Lee CS, Jones D, Harnett GB, Armstrong BK, Clark JR, Milross CG, Kim J, O'Brien CJ. Human papillomavirus predicts outcome in oropharyngeal cancer in patients treated primarily with surgery or radiation therapy. Br J Cancer. 2010;103(10):1510–1517. doi: 10.1038/sj.bjc.6605944. - DOI - PMC - PubMed
-
- Maxwell JH, Kumar B, Feng FY, Worden FP, Lee JS, Eisbruch A, Wolf GT, Prince ME, Moyer JS, Teknos TN. Tobacco use in human papillomavirus-positive advanced oropharynx cancer patients related to increased risk of distant metastases and tumor recurrence. Clin Cancer Res. 2010;16(4):1226–1235. doi: 10.1158/1078-0432.CCR-09-2350. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
Miscellaneous
