

Effectiveness of robust optimization in intensity-modulated proton therapy planning for head and neck cancers
- PMID: 23635259
- PMCID: PMC3651255
- DOI: 10.1118/1.4801899
Effectiveness of robust optimization in intensity-modulated proton therapy planning for head and neck cancers
Abstract
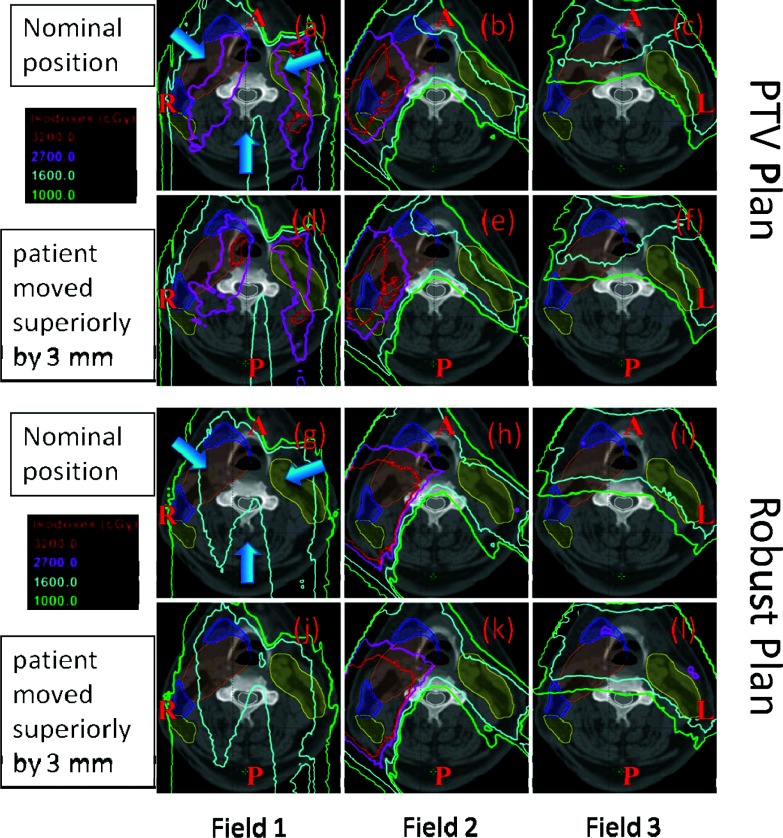
Purpose: Intensity-modulated proton therapy (IMPT) is highly sensitive to uncertainties in beam range and patient setup. Conventionally, these uncertainties are dealt using geometrically expanded planning target volume (PTV). In this paper, the authors evaluated a robust optimization method that deals with the uncertainties directly during the spot weight optimization to ensure clinical target volume (CTV) coverage without using PTV. The authors compared the two methods for a population of head and neck (H&N) cancer patients.
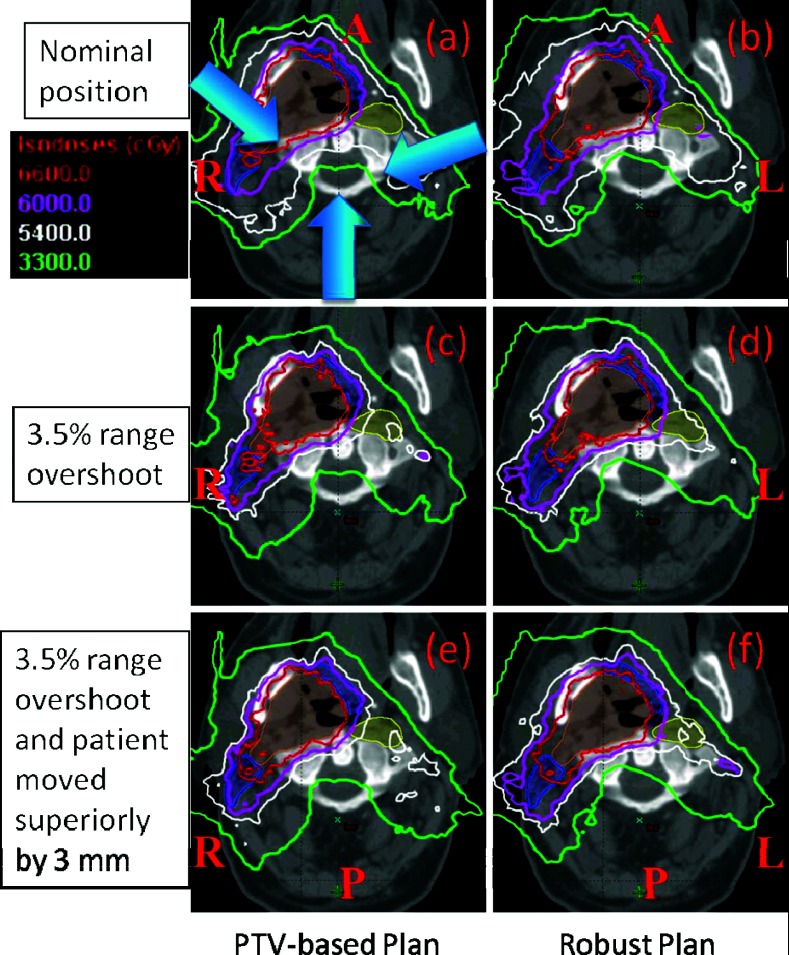
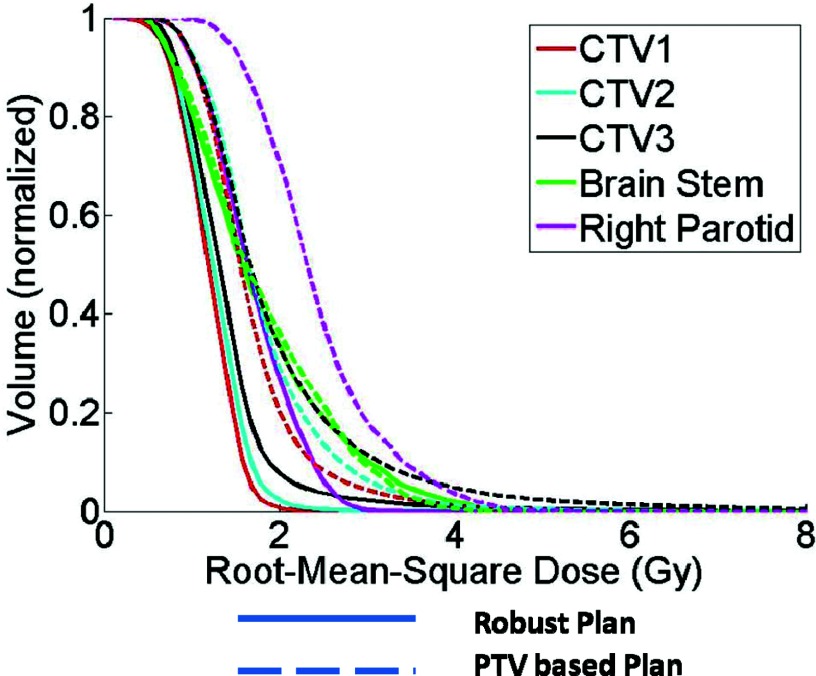
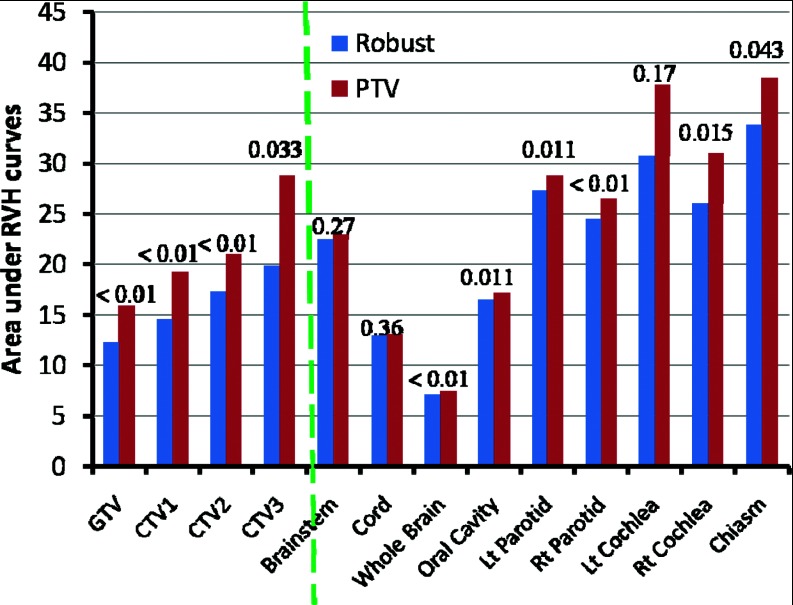
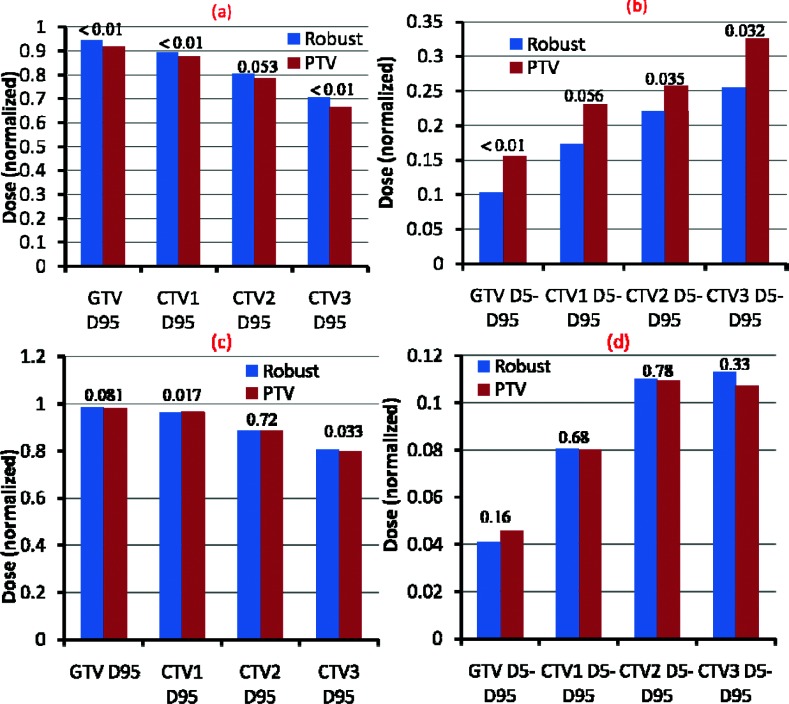
Methods: Two sets of IMPT plans were generated for 14 H&N cases, one being PTV-based conventionally optimized and the other CTV-based robustly optimized. For the PTV-based conventionally optimized plans, the uncertainties are accounted for by expanding CTV to PTV via margins and delivering the prescribed dose to PTV. For the CTV-based robustly optimized plans, spot weight optimization was guided to reduce the discrepancy in doses under extreme setup and range uncertainties directly, while delivering the prescribed dose to CTV rather than PTV. For each of these plans, the authors calculated dose distributions under various uncertainty settings. The root-mean-square dose (RMSD) for each voxel was computed and the area under the RMSD-volume histogram curves (AUC) was used to relatively compare plan robustness. Data derived from the dose volume histogram in the worst-case and nominal doses were used to evaluate the plan optimality. Then the plan evaluation metrics were averaged over the 14 cases and were compared with two-sided paired t tests.
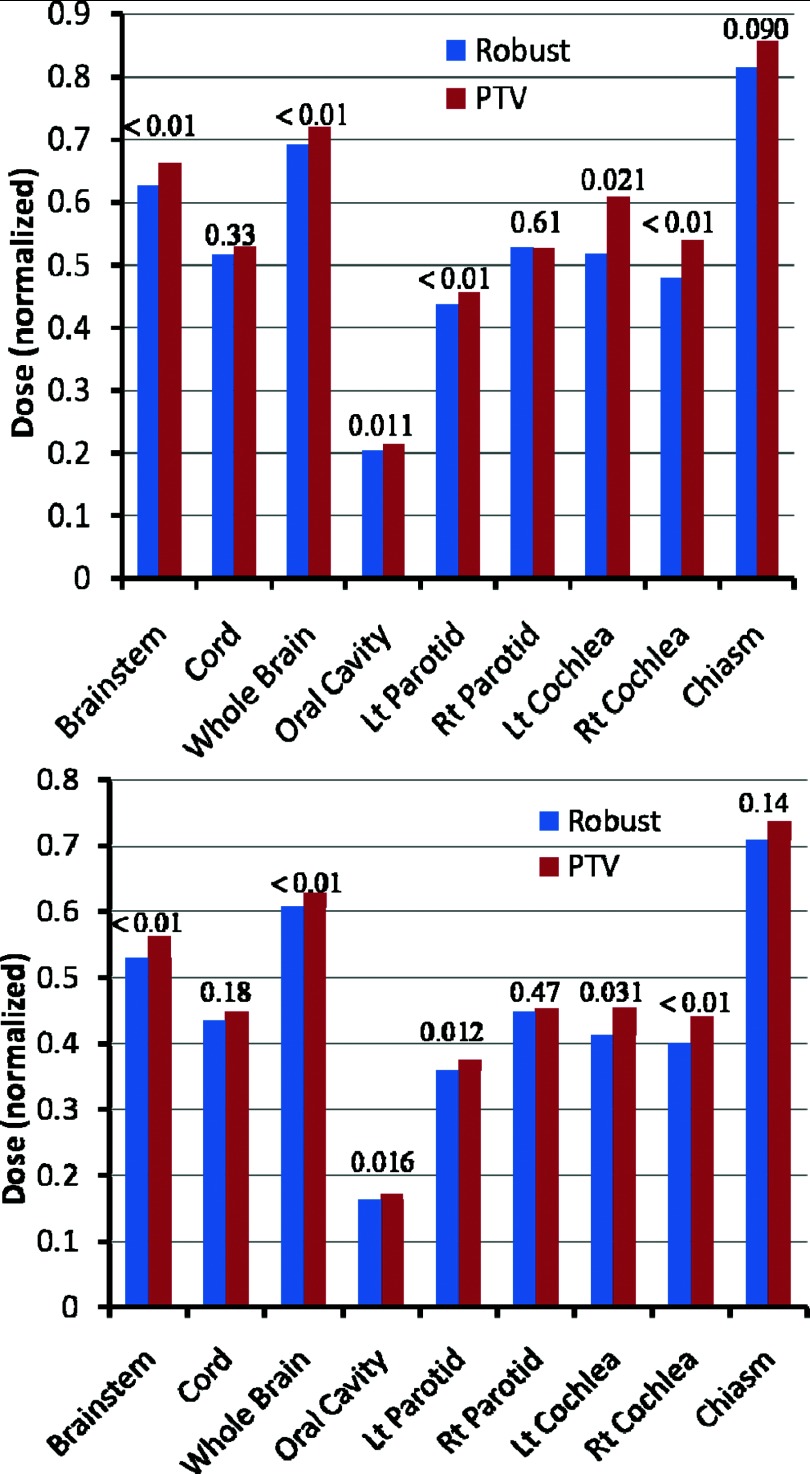
Results: CTV-based robust optimization led to more robust (i.e., smaller AUCs) plans for both targets and organs. Under the worst-case scenario and the nominal scenario, CTV-based robustly optimized plans showed better target coverage (i.e., greater D95%), improved dose homogeneity (i.e., smaller D5% - D95%), and lower or equivalent dose to organs at risk.
Conclusions: CTV-based robust optimization provided significantly more robust dose distributions to targets and organs than PTV-based conventional optimization in H&N using IMPT. Eliminating the use of PTV and planning directly based on CTV provided better or equivalent normal tissue sparing.
Figures
References
-
- Widesott L., Pierelli A., Fiorino C., Dell’Oca I., Broggi S., Catraneo G. M., Di Muzio N., Fazio F., Calandrino R., and Schwarz M., “Intensity-modulated proton therapy versus helical tomotherapy in nasopharynx cancer: Planning comparison and NTCP evaluation,” Int. J. Radiat. Oncol., Biol., Phys. 72, 589–596 (2008). 10.1016/j.ijrobp.2008.05.065 - DOI - PubMed
-
- Lomax A. J., Pedroni E., Rutz H., and Goitein G., “The clinical potential of intensity modulated proton therapy,” Z. Med. Phys. 14, 147–152 (2004). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
