

A novel dose-based positioning method for CT image-guided proton therapy
- PMID: 23635262
- PMCID: PMC3651206
- DOI: 10.1118/1.4801910
A novel dose-based positioning method for CT image-guided proton therapy
Abstract
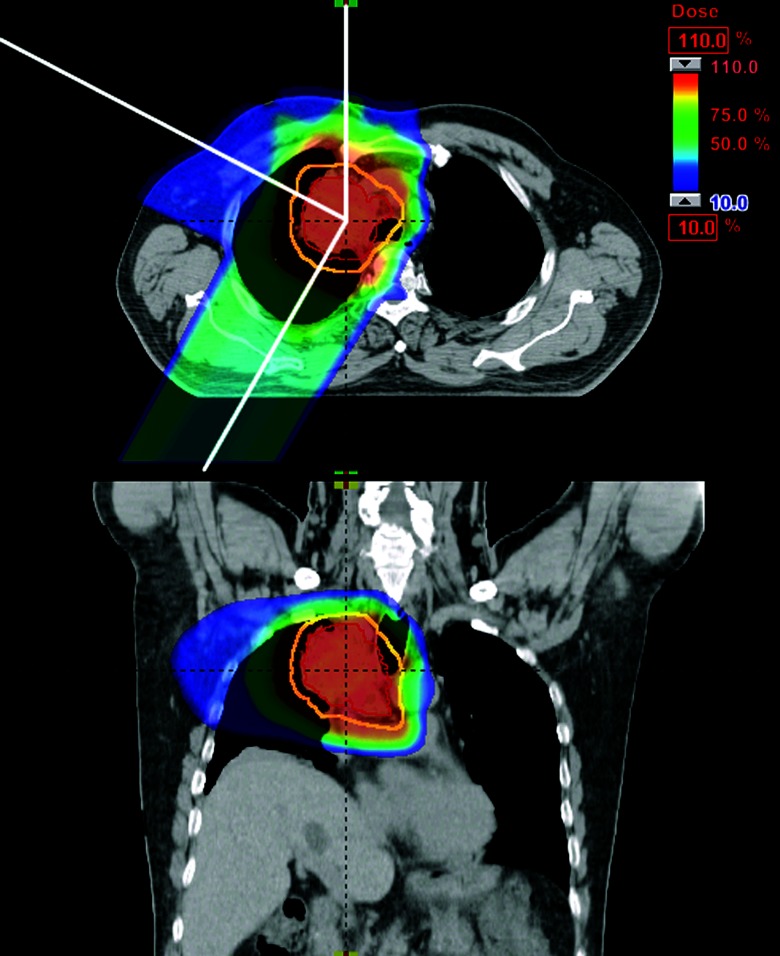
Purpose: Proton dose distributions can potentially be altered by anatomical changes in the beam path despite perfect target alignment using traditional image guidance methods. In this simulation study, the authors explored the use of dosimetric factors instead of only anatomy to set up patients for proton therapy using in-room volumetric computed tomographic (CT) images.
Methods: To simulate patient anatomy in a free-breathing treatment condition, weekly time-averaged four-dimensional CT data near the end of treatment for 15 lung cancer patients were used in this study for a dose-based isocenter shift method to correct dosimetric deviations without replanning. The isocenter shift was obtained using the traditional anatomy-based image guidance method as the starting position. Subsequent isocenter shifts were established based on dosimetric criteria using a fast dose approximation method. For each isocenter shift, doses were calculated every 2 mm up to ± 8 mm in each direction. The optimal dose alignment was obtained by imposing a target coverage constraint that at least 99% of the target would receive at least 95% of the prescribed dose and by minimizing the mean dose to the ipsilateral lung.
Results: The authors found that 7 of 15 plans did not meet the target coverage constraint when using only the anatomy-based alignment. After the authors applied dose-based alignment, all met the target coverage constraint. For all but one case in which the target dose was met using both anatomy-based and dose-based alignment, the latter method was able to improve normal tissue sparing.
Conclusions: The authors demonstrated that a dose-based adjustment to the isocenter can improve target coverage and/or reduce dose to nearby normal tissue.
Figures





References
-
- Chang J. Y., Zhang X., Wang X., Kang Y., Riley B., Bilton S., Mohan R., Komaki R., and Cox J. D., “Significant reduction of normal tissue dose by proton radiotherapy compared with three-dimensional conformal or intensity-modulated radiation therapy in Stage I or Stage III non-small-cell lung cancer,” Int. J. Radiat. Oncol. Biol. Phys. 65, 1087–1096 (2006). 10.1016/j.ijrobp.2006.01.052 - DOI - PubMed
-
- van Rooijen D. C., van Wieringen N., Stippel G., Crezee J., Koning C. C. E., and Bel A., “Dose-guided radiotherapy: Potential benefit of online dose recalculation for stereotactic lung irradiation in patients with non-small-cell lung cancer,” Int. J. Radiat. Oncol. Biol. Phys. 83, e557–e562 (2012). 10.1016/j.ijrobp.2011.12.055 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
