

Nonsurgical management of heavy menstrual bleeding: a systematic review
- PMID: 23635628
- PMCID: PMC4414119
- DOI: 10.1097/AOG.0b013e3182839e0e
Nonsurgical management of heavy menstrual bleeding: a systematic review
Abstract
Objective: To compare the effectiveness of nonsurgical abnormal uterine bleeding treatments for bleeding control, quality of life (QOL), pain, sexual health, patient satisfaction, additional treatments needed, and adverse events.
Data sources: MEDLINE, Cochrane databases, and Clinicaltrials.gov were searched from inception to May 2012. We included randomized controlled trials of nonsurgical treatments for abnormal uterine bleeding presumed secondary to endometrial dysfunction and abnormal uterine bleeding presumed secondary to ovulatory dysfunction. Interventions included the levonorgestrel intrauterine system, combined oral contraceptive pills (OCPs), progestins, nonsteroidal anti-inflammatory drugs (NSAIDs), and antifibrinolytics. Gonadotropin-releasing hormone agonists, danazol, and placebo were allowed as comparators.
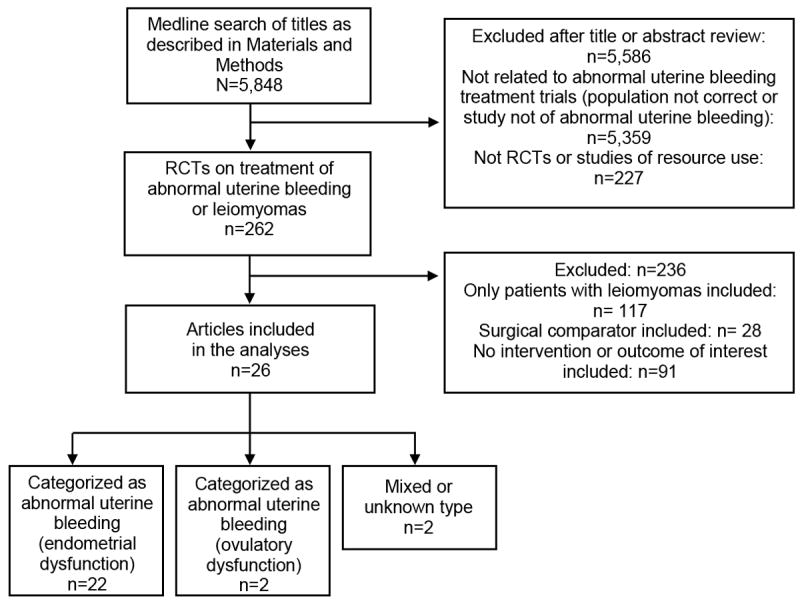
Methods of study selection: Two reviewers independently screened 5,848 citations and extracted eligible trials. Studies were assessed for quality and strength of evidence.
Tabulation, integration, and results: Twenty-six articles met inclusion criteria. For reduction of menstrual bleeding in women with abnormal uterine bleeding presumed secondary to endometrial dysfunction, the levonorgestrel intrauterine system (71-95% reduction), combined OCPs (35-69% reduction), extended cycle oral progestins (87% reduction), tranexamic acid (26-54% reduction), and NSAIDs (10-52% reduction) were all effective treatments. The levonorgestrel intrauterine system, combined OCPs, and antifibrinolytics were all superior to luteal-phase progestins (20% increase in bleeding to 67% reduction). The levonorgestrel intrauterine system was superior to combined OCPs and NSAIDs. Antifibrinolytics were superior to NSAIDs for menstrual bleeding reduction. Data were limited on other important outcomes such as QOL for women with abnormal uterine bleeding presumed secondary to endometrial dysfunction and for all outcomes for women with abnormal uterine bleeding presumed secondary to ovulatory dysfunction.
Conclusion: For the reduction in mean blood loss in women with heavy menstrual bleeding presumed secondary to abnormal uterine bleeding presumed secondary to endometrial dysfunction, we recommend the use of the levonorgestrel intrauterine system over OCPs, luteal-phase progestins, and NSAIDs. For other outcomes (QOL, pain, sexual health, patient satisfaction, additional treatments needed, and adverse events) and for treatment of abnormal uterine bleeding presumed secondary to ovulatory dysfunction, we were unable to make recommendations based on the limited available data.
Conflict of interest statement
Figures
Comment in
-
Review: levonorgestrel IU system, OCPs, and antifibrinolytics each reduce bleeding in endometrial dysfunction.Ann Intern Med. 2013 Sep 17;159(6):JC10. doi: 10.7326/0003-4819-159-6-201309170-02010. Ann Intern Med. 2013. PMID: 24042381 No abstract available.
References
-
- Liu Z, Doan QV, Blumenthal P, Dubois RW. A systematic review evaluating health-related quality of life, work impairment, and health care costs and utilization in abnormal uterine bleeding. Value Health. 2007;10(3):173–82. - PubMed
-
- Munro MG, Critchley HO, Fraser IS. The FIGO classification of causes of abnormal uterine bleeding: Malcolm G. Munro, Hilary O.D. Crithcley, Ian S. Fraser, for the FIGO Working Group on Menstrual Disorders. Int J Gynaecol Obstet. 2011;113(1):1–2. - PubMed
-
- Counsell C. Formulating questions and locating primary studies for inclusion in systematic reviews. Ann Intern Med. 1997;127(5):380–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
