

Long-term mortality associated with oophorectomy compared with ovarian conservation in the nurses' health study
- PMID: 23635669
- PMCID: PMC4254662
- DOI: 10.1097/AOG.0b013e3182864350
Long-term mortality associated with oophorectomy compared with ovarian conservation in the nurses' health study
Abstract
Objective: To report long-term mortality after oophorectomy or ovarian conservation at the time of hysterectomy in subgroups of women based on age at the time of surgery, use of estrogen therapy, presence of risk factors for coronary heart disease, and length of follow-up.
Methods: This was a prospective cohort study of 30,117 Nurses' Health Study participants undergoing hysterectomy for benign disease. Multivariable adjusted hazard ratios for death from coronary heart disease, stroke, breast cancer, epithelial ovarian cancer, lung cancer, colorectal cancer, total cancer, and all causes were determined comparing bilateral oophorectomy (n=16,914) with ovarian conservation (n=13,203).
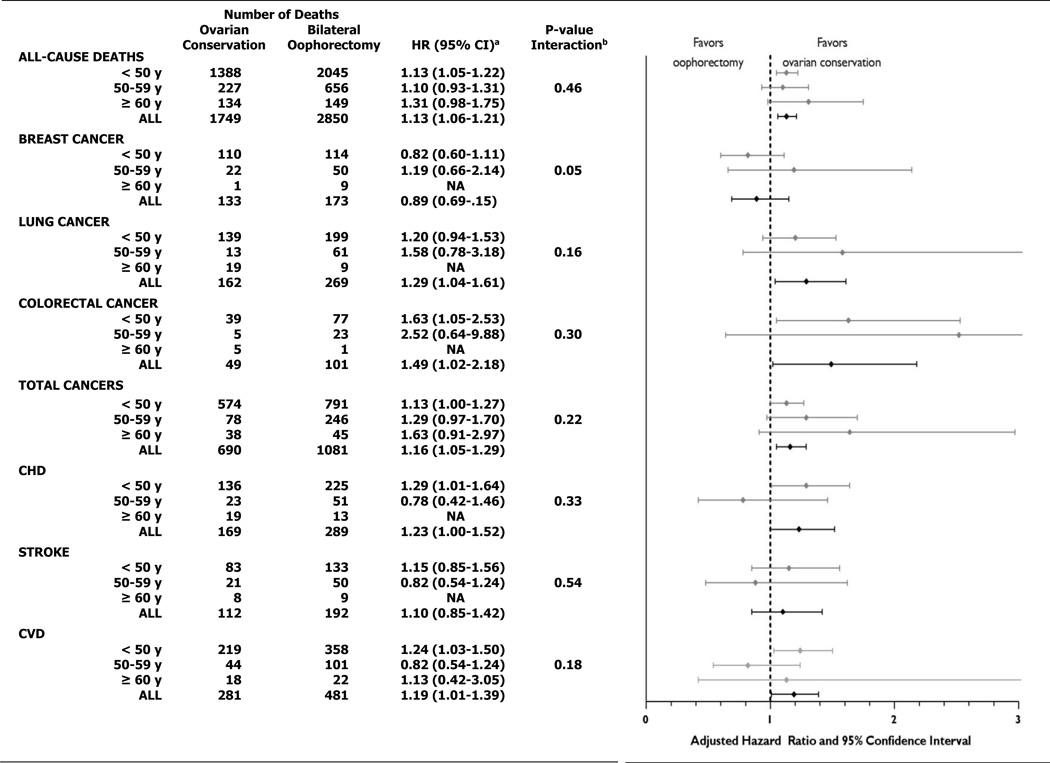
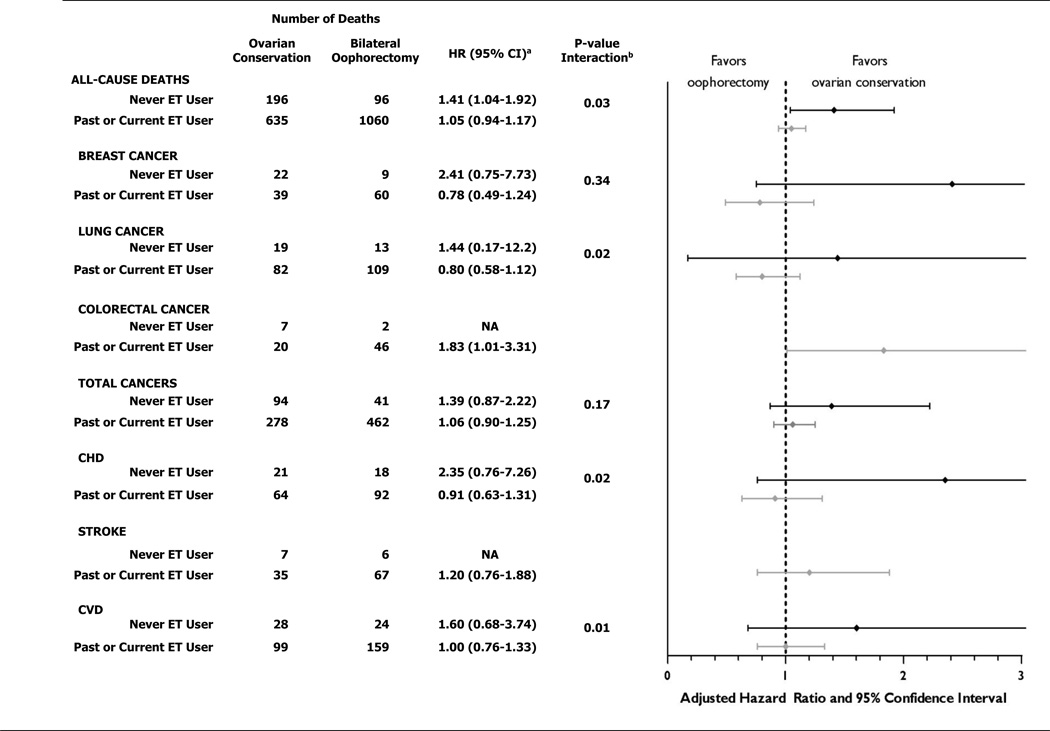
Results: Over 28 years of follow-up, 16.8% of women with hysterectomy and bilateral oophorectomy died from all causes compared with 13.3% of women who had ovarian conservation (hazard ratio 1.13, 95% confidence interval 1.06-1.21). Oophorectomy was associated with a lower risk of death from ovarian cancer (four women with oophorectomy compared with 44 women with ovarian conservation) and, before age 47.5 years, a lower risk of death from breast cancer. However, at no age was oophorectomy associated with a lower risk of other cause-specific or all-cause mortality. For women younger than 50 years at the time of hysterectomy, bilateral oophorectomy was associated with significantly increased mortality in women who had never used estrogen therapy but not in past and current users: assuming a 35-year lifespan after oophorectomy: number needed to harm for all-cause death=8, coronary heart disease death=33, and lung cancer death=50.
Conclusions: Bilateral oophorectomy is associated with increased mortality in women aged younger than 50 years who never used estrogen therapy and at no age is oophorectomy associated with increased survival.
Level of evidence: I.
Figures
Comment in
-
Ovaries, estrogen, and longevity.Obstet Gynecol. 2013 Apr;121(4):701-702. doi: 10.1097/AOG.0b013e31828af732. Obstet Gynecol. 2013. PMID: 23635666 No abstract available.
-
Long-term mortality associated with oophorectomy compared with ovarian conservation in the Nurses' Health Study.Obstet Gynecol. 2013 Aug;122(2 Pt 1):395-396. doi: 10.1097/AOG.0b013e31829d4376. Obstet Gynecol. 2013. PMID: 23969817 No abstract available.
-
In reply.Obstet Gynecol. 2013 Aug;122(2 Pt 1):396. doi: 10.1097/AOG.0b013e31829d438c. Obstet Gynecol. 2013. PMID: 23969818 No abstract available.
-
Ovaries, estrogen, and longevity and long-term mortality associated with oophorectomy compared with ovarian conservation in the Nurses' Health Study and variation in ovarian conservation in women undergoing hysterectomy for benign indications.Obstet Gynecol. 2013 Aug;122(2 Pt 1):397-398. doi: 10.1097/AOG.0b013e31829e3325. Obstet Gynecol. 2013. PMID: 23969821 No abstract available.
References
-
- Whiteman MK, Hillis SD, Jamieson DJ, Morrow B, Podgornik MN, Brett KM, Marchbanks PA. Inpatient hysterectomy surveillance in the United States, 2000–2004. Am J Obstet Gynecol. 2008;198:34.e1–37.e1. - PubMed
-
- Asante A, Whiteman MK, Kulkarni A, Cox S, Marchbanks PA, Jamieson DJ. Elective oophorectomy in the United States: trends and in-hospital complications, 1998–2006. Obstet Gynecol. 2010;116:1088–1095. - PubMed
-
- Colditz GA, Willett WC, Stampfer MJ, Rosner B, Speizer FE, Hennekens CH. Menopause and the risk of coronary heart disease in women. N Engl J Med. 1987;316:1105–1110. - PubMed
-
- Rocca WA, Grossardt BR, de Andrade M, Malkasian GD, Melton LJ., 3rd Survival patterns after oophorectomy in premenopausal women: a population-based cohort study. Lancet Oncol. 2006;7:821–828. - PubMed
-
- Jacoby VL, Grady D, Wactawski-Wende J, Manson JE, Allison MA, Kuppermann M, Sarto GE, Robbins J, Phillips L, Martin LW, O'Sullivan MJ, Jackson R, Rodabough RJ, Stefanick ML. Oophorectomy vs ovarian conservation with hysterectomy: cardiovascular disease, hip fracture, and cancer in the Women's Health Initiative Observational Study. Arch Intern Med. 2011;171:760–768. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
