

Impaired ultrasonographic cervical assessment after voiding: a randomized controlled trial
- PMID: 23635680
- PMCID: PMC3710113
- DOI: 10.1097/AOG.0b013e3182860b8d
Impaired ultrasonographic cervical assessment after voiding: a randomized controlled trial
Abstract
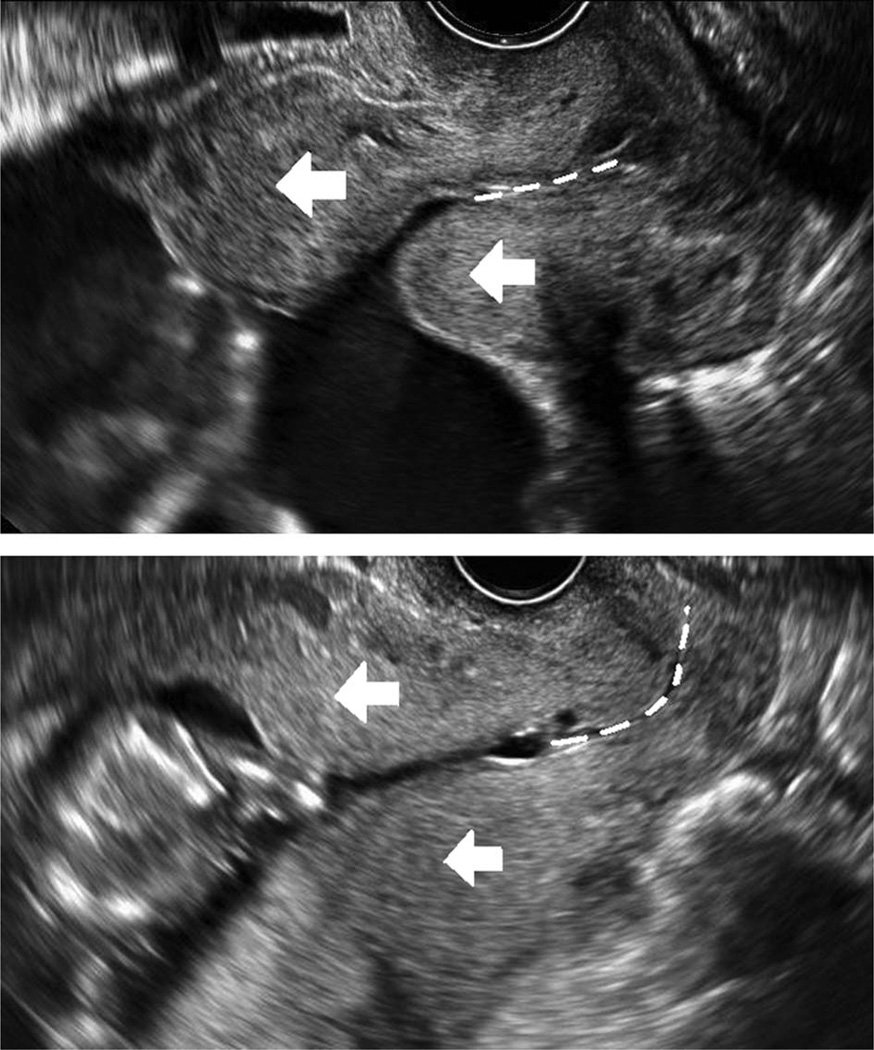
Objective: To estimate whether the timing of bladder emptying affects focal myometrial contraction development and image adequacy.
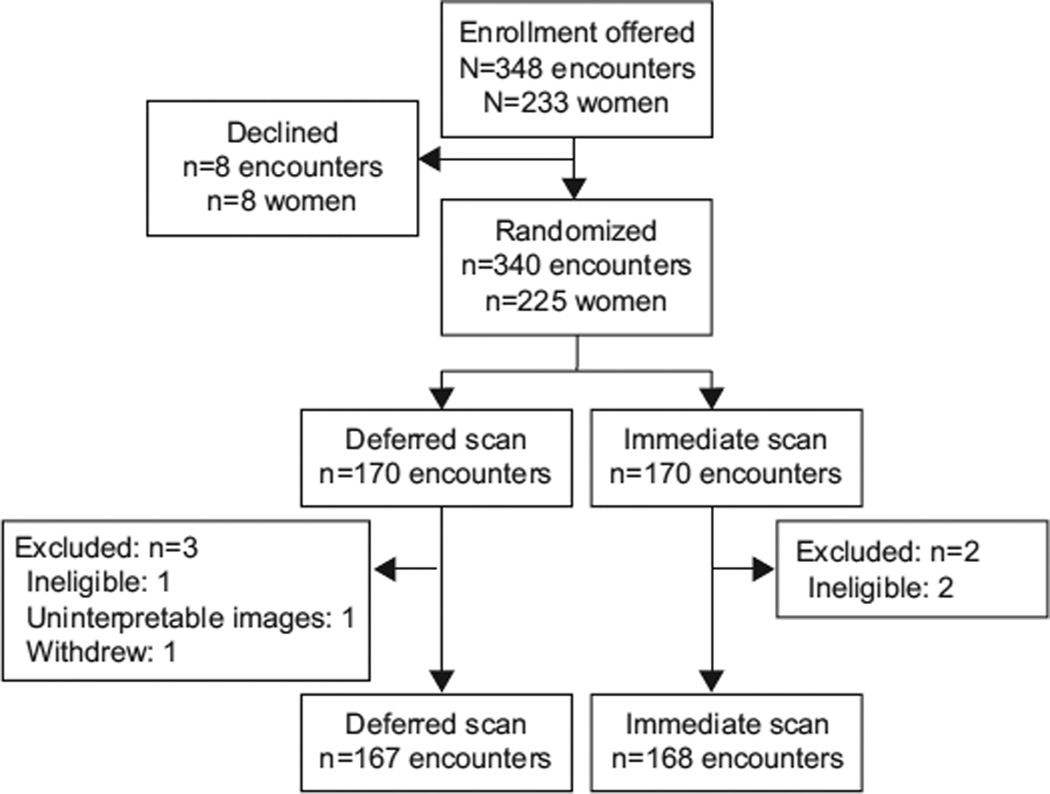
Methods: Women at 14 0/7-32 0/7 weeks of gestation undergoing a transvaginal ultrasound examination from January 1, 2012, to September 1, 2012, were eligible for this blinded randomized controlled trial. Participants were randomly assigned to undergo transvaginal imaging immediately after urination (within 5 minutes) or to defer the imaging by at least 15 minutes. The primary outcome was focal myometrial contraction development as determined by two independent blinded reviews of the images. Secondary outcomes included image adequacy and the diagnosis of placenta previa. Relative risks (RRs) and 95% confidence intervals (CIs) were calculated using repeated-measures log binomial regression.
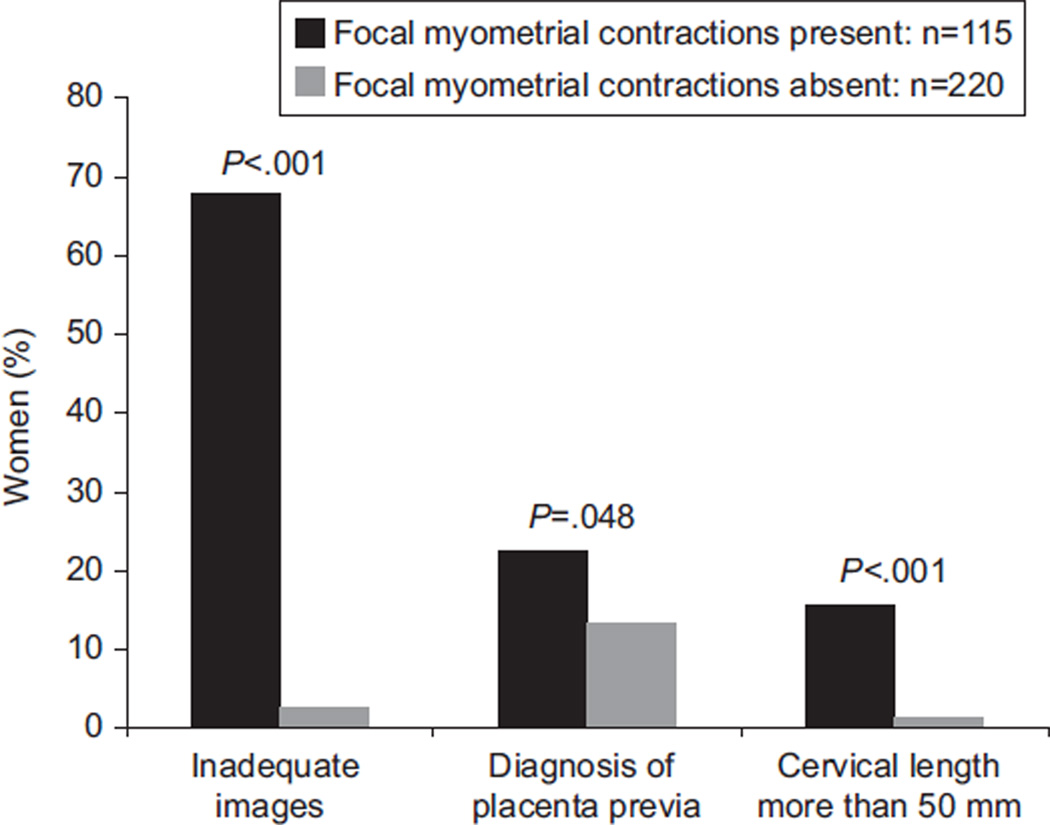
Results: Two hundred twenty-one women provided 335 randomized encounters for analysis. Women in the deferred scan group were 30% less likely to experience a focal myometrial contraction (28.1% compared with 40.5%, RR 0.70, 95% CI 0.52-0.93) and 41% less likely to have inadequate images (18.6% compared with 31.5%, RR 0.59, 95% CI 0.40-0.86). The two groups were equally likely to be diagnosed with placenta previa (P=.13). However, participants in the deferred scan group were 76% less likely to have images demonstrating a placenta previa and focal myometrial contraction (3.0% compared with 12.5%, RR 0.24, 95% CI 0.09-0.62) than participants in the immediate scan group. Eight women would need to defer imaging for 15 minutes from bladder voiding to prevent one focal myometrial contraction of the lower uterine segment or inadequate imaging.
Conclusions: A brief interval (at least 15 minutes) between voiding and transvaginal cervical evaluation is associated with decreased risk for focal myometrial contractions and improved imaging.
Clinical trial registration: ClinicalTrials.gov, www.clinicaltrials.gov, NCT01513395.
Level of evidence: I.
Conflict of interest statement
The authors did not report any potential conflicts of interest.
Figures
References
-
- Iams JD, Goldenberg RL, Meis PJ, Mercer BM, Moawad A, Das A, et al. The length of the cervix and the risk of spontaneous premature delivery. N Engl J Med. 1996;334:567–572. - PubMed
-
- Owen J, Yost N, Berghella V, Thom E, Swain M, Dildy GA, 3rd, et al. Mid-trimester endovaginal sonography in women at high risk for spontaneous preterm birth. JAMA. 2001;286:1340–1348. - PubMed
-
- Berghella V, Tolosa JE, Kuhlman D, Weiner S, Bolognese RJ, Wapner RJ. Cervical ultrasonography compared with manual examination as a predictor of preterm delivery. Am J Obstet Gynecol. 1997;177:723–730. - PubMed
-
- Sherman SJ, Carlson DE, Platt LD, Medearis AL. Transvaginal ultrasound: does it help in the diagnosis of placenta previa? Ultrasound Obstet Gynecol. 1992;2:256–260. - PubMed
-
- Taipale P, Hiilesmaa V, Ylöstalo P. Diagnosis of placenta previa by transvaginal sonographic screening at 12–16 weeks in a nonselected population. Obstet Gynecol. 1997;89:364–367. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
