

Risk of oophorectomy after hysterectomy
- PMID: 23635745
- PMCID: PMC3810957
- DOI: 10.1097/AOG.0b013e31828e89df
Risk of oophorectomy after hysterectomy
Abstract
Objective: To compare the risk of subsequent oophorectomy among women who underwent hysterectomy for benign indications and those who did not.
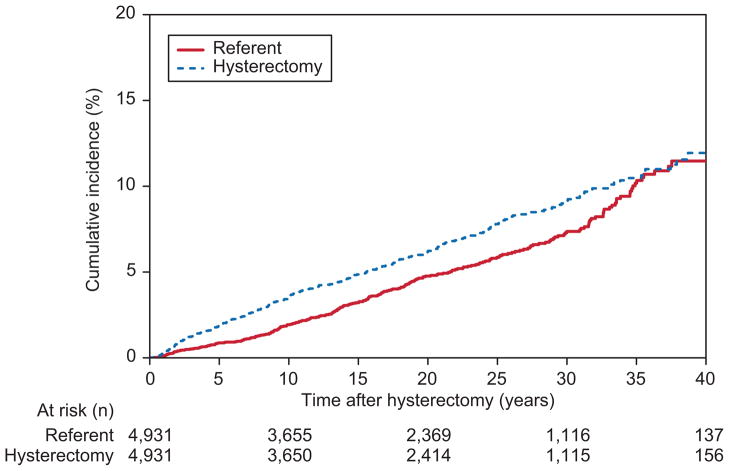
Methods: Using Rochester Epidemiology Project resources, we compared the risk of oophorectomy through December 31, 2008, among 4,931 women in Olmsted County, Minnesota, who underwent ovary-sparing hysterectomy for benign indications (case group) between 1965 and 2002, with 4,931 age-matched women who did not undergo hysterectomy (referent group). The cumulative incidence of subsequent oophorectomy was estimated by the Kaplan-Meier method, and comparisons were evaluated by Cox proportional hazard models using age as the time scale to allow for complete age adjustment.
Results: The median follow-up times for case group and referent group participants were 19.6 and 19.4 years, respectively. At 10, 20, and 30 years after hysterectomy, the respective cumulative incidences of subsequent oophorectomy were 3.5%, 6.2%, and 9.2% among case group participants and 1.9%, 4.8%, and 7.3% among referent group participants. The overall risk of subsequent oophorectomy among case group participants was significantly higher than among referent group participants (hazard ratio [HR] 1.20, 95% confidence interval [CI] 1.02-1.42; P=.03). Furthermore, among case group participants, the risk of subsequent oophorectomy was significantly higher (HR 2.15, 95% CI 1.51-3.07; P<.001) in women who had both ovaries preserved compared with those who initially had one ovary preserved.
Conclusion: The incidence of oophorectomy after hysterectomy is only 9.2% at 30-year follow-up and is only 1.9 percentage points higher than the incidence of oophorectomy in referent women with intact reproductive organs.
Level of evidence: II.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Parker WH, Broder MS, Liu Z, Shoupe D, Farquhar C, Berek JS. Ovarian conservation at the time of hysterectomy for benign disease. Clin Obstet Gynecol. 2007 Jun;50(2):354–61. - PubMed
-
- Christ JE, Lotze EC. The residual ovary syndrome. Obstet Gynecol. 1975 Nov;46(5):551–6. - PubMed
-
- Naylor AC. Hysterectomy: analysis of 2,901 personally performed procedures. S Afr Med J. 1984 Feb 18;65(7):242–5. - PubMed
-
- Rocca WA, Grossardt BR, de Andrade M, Malkasian GD, Melton LJ., 3rd Survival patterns after oophorectomy in premenopausal women: a population-based cohort study. Lancet Oncol. 2006 Oct;7(10):821–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
