

Cost-effectiveness of nurse practitioner/community health worker care to reduce cardiovascular health disparities
- PMID: 23635809
- PMCID: PMC3766479
- DOI: 10.1097/JCN.0b013e3182945243
Cost-effectiveness of nurse practitioner/community health worker care to reduce cardiovascular health disparities
Abstract
Background: Although evidence-based guidelines on the management of cardiovascular disease (CVD) and type 2 diabetes have been widely published, implementation of recommended therapies is suboptimal.
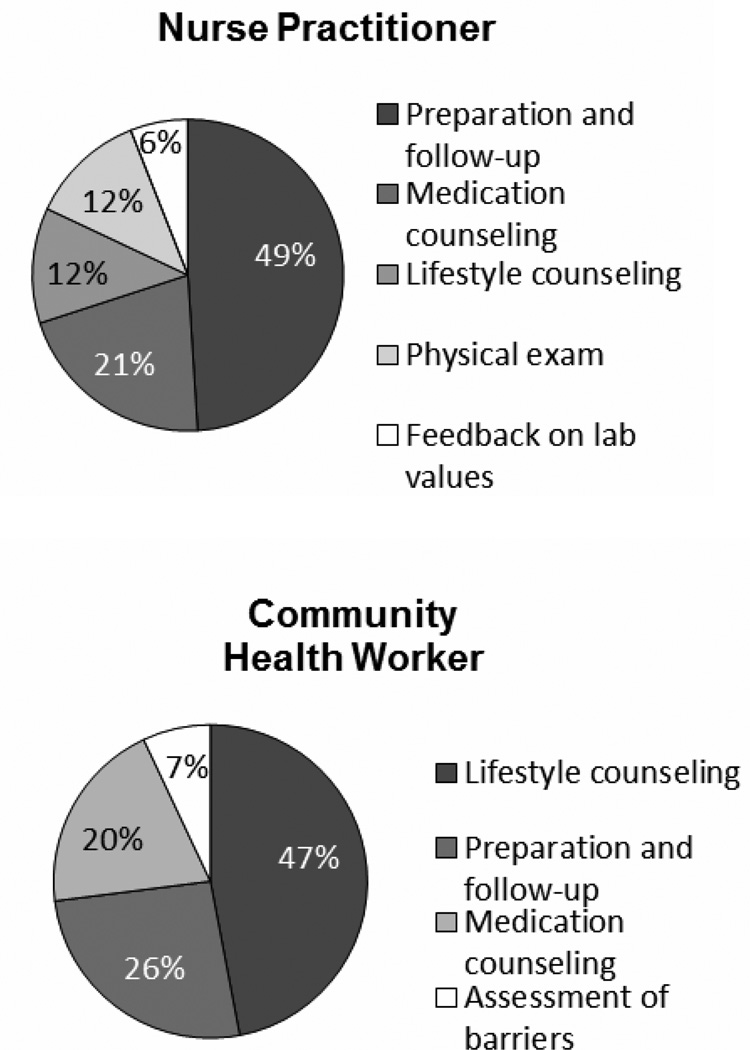
Objective: The aim of this study was to evaluate the cost-effectiveness of a comprehensive program of CVD risk reduction delivered by nurse practitioner/community health worker (NP/CHW) teams versus enhanced usual care to improve lipids, blood pressure (BP), and hemoglobin (Hb) A1c levels in patients in urban community health centers.
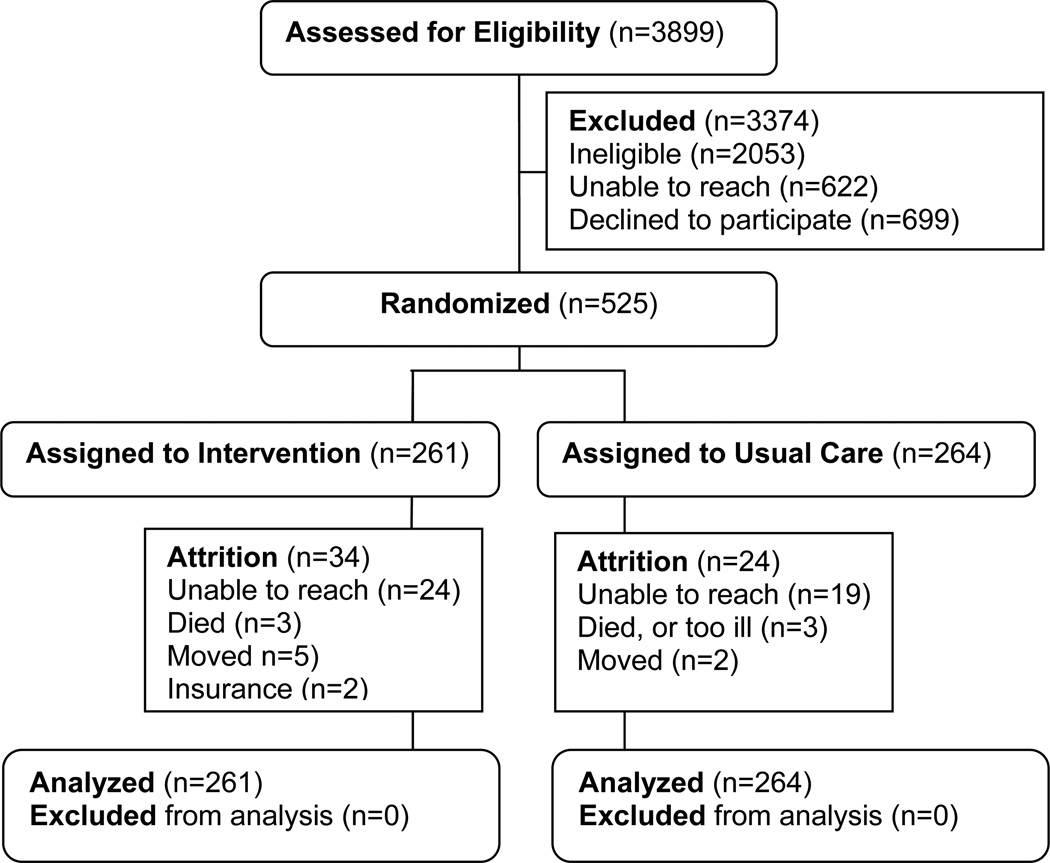
Methods: A total of 525 patients with documented CVD, type 2 diabetes, hypercholesterolemia, or hypertension and levels of low-density lipoprotein cholesterol, BP, or Hb A1c that exceeded goals established by national guidelines were randomized to NP/CHW (n = 261) or enhanced usual care (n = 264) groups. Cost-effectiveness ratios were calculated, determining costs per percent and unit change in the primary outcomes.
Results: The mean incremental total cost per patient (NP/CHW and physician) was only $627 (confidence interval, 248-1015). The cost-effectiveness of the 1-year intervention was $157 for every 1% drop in systolic BP and $190 for every 1% drop in diastolic BP, $149 per 1% drop in Hb A1c, and $40 per 1% drop in low-density lipoprotein cholesterol.
Conclusions: The findings suggest that management by an NP/CHW team is a cost-effective approach for community health centers to consider in improving the care of patients with existing CVD or at high risk for the development of CVD.
Figures
Similar articles
-
Community Outreach and Cardiovascular Health (COACH) Trial: a randomized, controlled trial of nurse practitioner/community health worker cardiovascular disease risk reduction in urban community health centers.Circ Cardiovasc Qual Outcomes. 2011 Nov 1;4(6):595-602. doi: 10.1161/CIRCOUTCOMES.111.961573. Epub 2011 Sep 27. Circ Cardiovasc Qual Outcomes. 2011. PMID: 21953407 Free PMC article. Clinical Trial.
-
COACH trial: a randomized controlled trial of nurse practitioner/community health worker cardiovascular disease risk reduction in urban community health centers: rationale and design.Contemp Clin Trials. 2011 May;32(3):403-11. doi: 10.1016/j.cct.2011.01.001. Epub 2011 Jan 15. Contemp Clin Trials. 2011. PMID: 21241828 Free PMC article. Clinical Trial.
-
Cost-effectiveness analysis of a cluster-randomized, culturally tailored, community health worker home-visiting diabetes intervention versus standard care in American Samoa.Hum Resour Health. 2019 Mar 5;17(1):17. doi: 10.1186/s12960-019-0356-6. Hum Resour Health. 2019. PMID: 30836964 Free PMC article. Clinical Trial.
-
Cost-effectiveness of nurse practitioner management of hypercholesterolemia following coronary revascularization.J Am Acad Nurse Pract. 2006 Sep;18(9):436-44. doi: 10.1111/j.1745-7599.2006.00159.x. J Am Acad Nurse Pract. 2006. PMID: 16958775 Clinical Trial.
-
Evaluation of Clinically Integrated Community Health Worker Support Interventions for Adults With Cardiovascular Disease: A Literature Review Guided by the PRISM Framework.Fam Community Health. 2025 Apr-Jun 01;48(2):144-177. doi: 10.1097/FCH.0000000000000422. Epub 2025 Jan 21. Fam Community Health. 2025. PMID: 39836517 Review.
Cited by
-
WHO-PEN intervention in Iran's health system based on 5As healthy lifestyle counseling model: A randomized-clinical trial.J Educ Health Promot. 2023 Jan 31;12:18. doi: 10.4103/jehp.jehp_107_22. eCollection 2023. J Educ Health Promot. 2023. PMID: 37034862 Free PMC article.
-
Racial disparities in stroke incidence in the Women's Health Initiative: Exploring biological, behavioral, psychosocial, and social risk factors.SSM Popul Health. 2023 Dec 3;25:101570. doi: 10.1016/j.ssmph.2023.101570. eCollection 2024 Mar. SSM Popul Health. 2023. PMID: 38313870 Free PMC article.
-
Knowledge and Attitudes of Potential Community Health Worker Employers: Findings from the State of Arkansas, USA.J Community Health. 2022 Apr;47(2):298-305. doi: 10.1007/s10900-021-01043-7. Epub 2021 Nov 24. J Community Health. 2022. PMID: 34817754
-
A Systematic Review of Community Health Center Based Interventions for People with Diabetes.J Community Health. 2019 Dec;44(6):1253-1280. doi: 10.1007/s10900-019-00693-y. Epub 2019 Jul 6. J Community Health. 2019. PMID: 31280431
-
Economics of Community Health Workers for Chronic Disease: Findings From Community Guide Systematic Reviews.Am J Prev Med. 2019 Mar;56(3):e95-e106. doi: 10.1016/j.amepre.2018.10.009. Am J Prev Med. 2019. PMID: 30777167 Free PMC article.
References
-
- Sokol MC, McGuigan KA, Verbrugge RR, Epstein RS. Impact of medication adherence on hospitalization risk and healthcare cost. Med Care. 2005;43:521–530. - PubMed
-
- Ho PM, Rumsfeld JS, Masoudi, et al. Effect of medication non-adherence on hospitalization and mortality among patients with diabetes mellitus. Archives of Internal Medicine. 2006;166(17):1836–1841. - PubMed
-
- Allen JK. Cholesterol management: an opportunity for nurse case managers. J Cardiovasc Nurs. 2000;14(2):50–58. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
