

Underestimation of adolescent obesity
- PMID: 23636345
- PMCID: PMC4006016
- DOI: 10.1097/NNR.0b013e318286b790
Underestimation of adolescent obesity
Abstract
Background: Previous studies assessing the validity of adolescent self-reported height and weight for estimating obesity prevalence have not accounted for, potential bias due to nonresponse in self-reports.
Objectives: The aim of this study was to assess the implications of selective nonresponse in self-reports of height and weight for estimates of adolescent obesity.
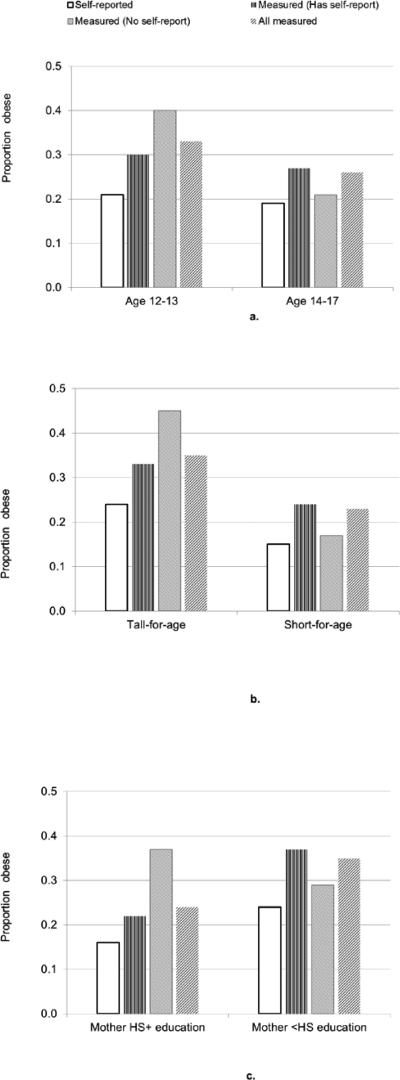
Methods: The authors analyzed 613 adolescents ages 12-17 years from the 2006-2008 Los Angeles Family and Neighborhood Survey, a longitudinal study of Los Angeles County households with an oversample of poor neighborhoods. Obesity prevalence estimates were compared based on (a) self-report, (b) measured height and weight for those who did report, and (c) measured height and weight for those who did report.
Results: Among younger teens, measured obesity prevalence was higher for those who did not report height and weight compared with those who did (40% vs. 30%). Consequently, obesity prevalence based on self-reported height and weight underestimated measured prevalence by 12 percentage points (when accounting for nonresponse) versus 9 percentage points (when nonresponse was not accounted for). Results were robust to the choice of difference child growth references.
Discussion: Adolescent obesity surveillance and prevention efforts must take into account selective nonresponse for self-reported height and weight, particularly for younger teens. Results should be replicated in a nationally representative sample.
Figures
Similar articles
-
Two-method measurement for adolescent obesity epidemiology: reducing the bias in self-report of height and weight.J Adolesc Health. 2013 Sep;53(3):322-7. doi: 10.1016/j.jadohealth.2013.03.026. Epub 2013 May 15. J Adolesc Health. 2013. PMID: 23684216 Free PMC article.
-
Does the use of prediction equations to correct self-reported height and weight improve obesity prevalence estimates? A pooled cross-sectional analysis of Health Survey for England data.BMJ Open. 2023 Jan 13;13(1):e061809. doi: 10.1136/bmjopen-2022-061809. BMJ Open. 2023. PMID: 36639207 Free PMC article.
-
Ethnic variation in validity of the estimated obesity prevalence using self-reported weight and height measurements.BMC Public Health. 2011 May 30;11:408. doi: 10.1186/1471-2458-11-408. BMC Public Health. 2011. PMID: 21624122 Free PMC article.
-
Accuracy of adolescent self-report of height and weight in assessing overweight status: a literature review.Arch Pediatr Adolesc Med. 2007 Dec;161(12):1154-61. doi: 10.1001/archpedi.161.12.1154. Arch Pediatr Adolesc Med. 2007. PMID: 18056560 Review.
-
A comparison of measured versus self-reported anthropometrics for assessing obesity in adults: a literature review.Scand J Public Health. 2018 Jul;46(5):565-579. doi: 10.1177/1403494818761971. Epub 2018 Mar 10. Scand J Public Health. 2018. PMID: 29528773 Review.
Cited by
-
Self-reported versus actual weight and height data contribute to different weight misperception classifications.South Med J. 2014 Jun;107(6):348-55. doi: 10.14423/01.SMJ.0000450708.52011.7c. South Med J. 2014. PMID: 24945166 Free PMC article.
-
Reliability of Self-Reported Height and Weight in Children: A School-Based Cross-Sectional Study and a Review.Nutrients. 2022 Dec 23;15(1):75. doi: 10.3390/nu15010075. Nutrients. 2022. PMID: 36615731 Free PMC article. Review.
-
Trends and correlates of unhealthy dieting behaviours among adolescents in the United States, 1999-2013.BMC Public Health. 2018 Apr 17;18(1):439. doi: 10.1186/s12889-018-5348-2. BMC Public Health. 2018. PMID: 29661180 Free PMC article.
-
The Accuracy of Self-Reported Body Weight Is High but Dependent on Recent Weight Change and Negative Affect in Teenage Girls.Int J Environ Res Public Health. 2020 Nov 6;17(21):8203. doi: 10.3390/ijerph17218203. Int J Environ Res Public Health. 2020. PMID: 33172095 Free PMC article.
-
The shape of things to come? Obesity prevalence among foreign-born vs. US-born Mexican youth in California.Soc Sci Med. 2013 Feb;78:1-8. doi: 10.1016/j.socscimed.2012.10.023. Epub 2012 Nov 6. Soc Sci Med. 2013. PMID: 23273875 Free PMC article.
References
-
- Adair LS. Child and adolescent obesity: epidemiology and developmental perspectives. Physiology & Behavior. 2008;94:8–16. - PubMed
-
- Akinbami LJ, Ogden CL. Childhood Overweight Prevalence in the United States: The Impact of Parent-reported Height and Weight. Obesity Research. 2009;17:1574–1580. - PubMed
-
- Brener ND, McManus T, Galuska DA, Lowry R, Wechsler H. Reliability and validity of self-reported height and weight among high school students. Journal of Adolescent Health. 2003;32:281–287. - PubMed
-
- Dauphinot V, Wolff H, Naudin F, Gueguen R, Sermet C, Gaspoz JM, Kossovsky MP. New obesity body mass index threshold for self-reported data. Journal of Epidemiology & Community Health. 2009;63:863–864. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
