

Avoiding hypoglycemia: a key to success for glucose-lowering therapy in type 2 diabetes
- PMID: 23637538
- PMCID: PMC3639216
- DOI: 10.2147/VHRM.S33934
Avoiding hypoglycemia: a key to success for glucose-lowering therapy in type 2 diabetes
Abstract
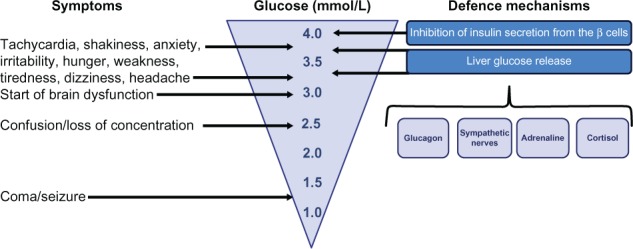
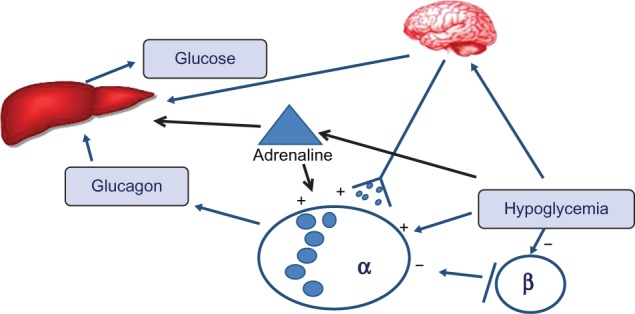
Type 2 diabetes carries a risk for hypoglycemia, particularly in patients on an intensive glucose control plan as a glucose-lowering strategy, where hypoglycemia may be a limitation for the therapy and also a factor underlying clinical inertia. Glucose-lowering medications that increase circulating insulin in a glucose-independent manner, such as insulin and sulfonylurea therapy, are the most common cause of hypoglycemia. However, other factors such as a delayed or missed meal, physical exercise, or drug or alcohol consumption may also contribute. Specific risk factors for development of hypoglycemia are old age, long duration of diabetes, some concomitant medication, renal dysfunction, hypoglycemia unawareness, and cognitive dysfunction. Hypoglycemia is associated with acute short-term symptoms related to either counterregulation, such as tachycardia and sweating, or to neuroglycopenia, such as irritability, confusion, and in severe cases stupor, coma, and even death. However, there are also long-term consequences of hypoglycemia such as reduced working capacity, weight gain, loss of self-confidence with reduced quality of life, and increased risk for cardiovascular diseases. For both the patients, the health care system, and the society at large, hypoglycemia carries a high cost. Strategies to mitigate the risk of hypoglycemia include awareness of the condition; education of patients, relatives, and health care providers; and selecting appropriate glucose-lowering medication that also judges the risk for hypoglycemia to prevent this complication. This article summarizes the current knowledge of hypoglycemia and its consequences with a special emphasis on its consequences for the choice of glucose-lowering therapy.
Keywords: hypoglycemia; incretin therapy; insulin; sulfonylurea; treatment; type 2 diabetes.
Figures
References
-
- Holman RR, Paul SK, Bethel MA, Matthews DR, Neil HA. 10-year follow-up of intensive glucose control in type 2 diabetes. N Engl J Med. 2008;359(15):1577–1589. - PubMed
-
- Rosenstock J, Dailey G, Massi-Benedetti M, Fritsche A, Lin Z, Salzman A. Reduced hypoglycemia risk with insulin glargine: a meta-analysis comparing insulin glargine with human NPH insulin in type 2 diabetes. Diabetes Care. 2005;28(4):950–955. - PubMed
-
- Barnett A. Dosing of insulin glargine in the treatment of type 2 diabetes. Clin Ther. 2007;29(6):987–999. - PubMed
-
- Zoungas S, Chalmers J, Kengne AP, et al. The efficacy of lowering glycated haemoglobin with a gliclazide modified release-based intensive glucose lowering regimen in the ADVANCE trial. Diabet Res Clin Pract. 2010;89(2):126–133. - PubMed
-
- Briscoe VJ, Danis SN. Hypoglycemia in type 1 and type 2 diabetes: physiology, pathophysiology and management. Clin Diabetes. 2006;24(3):115–121.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
