

Brainstem involvement as a cause of central sleep apnea: pattern of microstructural cerebral damage in patients with cerebral microangiopathy
- PMID: 23637744
- PMCID: PMC3634049
- DOI: 10.1371/journal.pone.0060304
Brainstem involvement as a cause of central sleep apnea: pattern of microstructural cerebral damage in patients with cerebral microangiopathy
Abstract
Background: The exact underlying pathomechanism of central sleep apnea with Cheyne-Stokes respiration (CSA-CSR) is still unclear. Recent studies have demonstrated an association between cerebral white matter changes and CSA. A dysfunction of central respiratory control centers in the brainstem was suggested by some authors. Novel MR-imaging analysis tools now allow far more subtle assessment of microstructural cerebral changes. The aim of this study was to investigate whether and what severity of subtle structural cerebral changes could lead to CSA-CSR, and whether there is a specific pattern of neurodegenerative changes that cause CSR. Therefore, we examined patients with Fabry disease (FD), an inherited, lysosomal storage disease. White matter lesions are early and frequent findings in FD. Thus, FD can serve as a "model disease" of cerebral microangiopathy to study in more detail the impact of cerebral lesions on central sleep apnea.
Patients and methods: Genetically proven FD patients (n = 23) and age-matched healthy controls (n = 44) underwent a cardio-respiratory polysomnography and brain MRI at 3.0 Tesla. We applied different MR-imaging techniques, ranging from semiquantitative measurement of white matter lesion (WML) volumes and automated calculation of brain tissue volumes to VBM of gray matter and voxel-based diffusion tensor imaging (DTI) analysis.
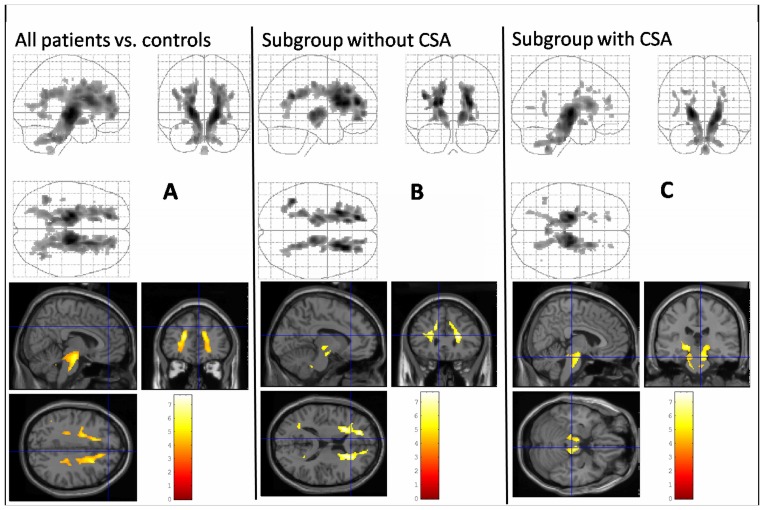
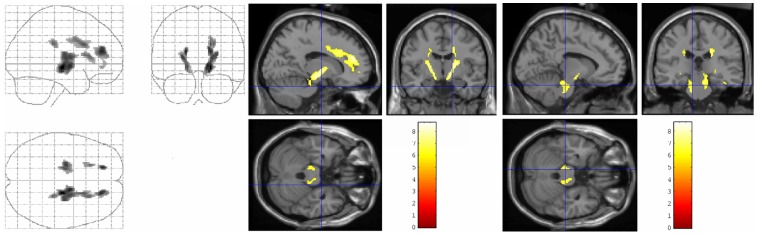
Results: In 5 of 23 Fabry patients (22%) CSA-CSR was detected. Voxel-based DTI analysis revealed widespread structural changes in FD patients when compared to the healthy controls. When calculated as a separate group, DTI changes of CSA-CSR patients were most prominent in the brainstem. Voxel-based regression analysis revealed a significant association between CSR severity and microstructural DTI changes within the brainstem.
Conclusion: Subtle microstructural changes in the brainstem might be a neuroanatomical correlate of CSA-CSR in patients at risk of WML. DTI is more sensitive and specific than conventional structural MRI and other advanced MR analyses tools in demonstrating these abnormalities.
Conflict of interest statement
Figures
References
-
- Iber C, Ancoli-Israel S, Chesson A, Quan SF, editors (2007) The AASM manual for the scoring of sleep and associated events: Rules, terminology, and technical specification. Westchester, IL: American Academy of Sleep Medicine.
-
- Yumino D, Bradley TD (2008) Central sleep apnea and cheyne-stokes respiration. Proceedings of the American Thoracic Society 5: 226–236. - PubMed
-
- Solin P, Roebuck T, Johns DP, Walters EH, Naughton MT (2000) Peripheral and central ventilatory responses in central sleep apnea with and without congestive heart failure. American Journal of Respiratory and Critical Care Medicine 162: 2194–2200. - PubMed
-
- Nopmaneejumruslers C, Kaneko Y, Hajek V, Zivanovic V, Bradley TD (2005) Cheyne-stokes respiration in stroke: Relationship to hypocapnia and occult cardiac dysfunction. American Journal of Respiratory and Critical Care Medicine 171: 1048–1052. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
