

Understanding providers' offering and patients' acceptance of HIV screening in emergency departments: a multilevel analysis. ANRS 95008, Paris, France
- PMID: 23638133
- PMCID: PMC3639277
- DOI: 10.1371/journal.pone.0062686
Understanding providers' offering and patients' acceptance of HIV screening in emergency departments: a multilevel analysis. ANRS 95008, Paris, France
Abstract
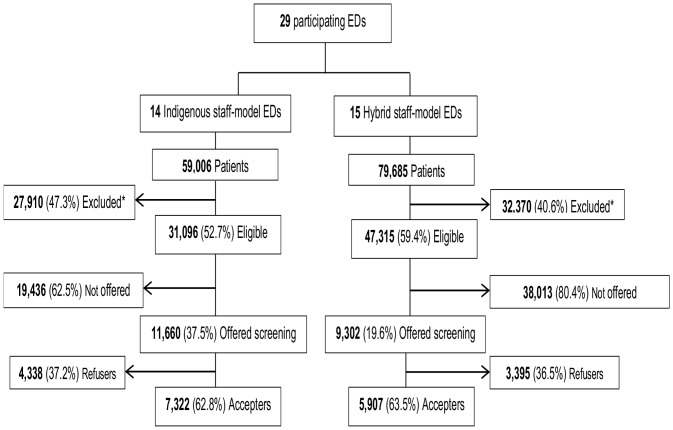
Objective: We assessed the EDs' characteristics associated with the offer and acceptance rates of a nontargeted HIV rapid-test screening in 29 Emergency Departments (EDs) in the metropolitan Paris region (11.7 million inhabitants), where half of France's new HIV cases are diagnosed annually.
Methods: EDs nurses offered testing to all patients 18-64-year-old, able to provide consent, either with or without supplemental staff (hybrid staff model or indigenous staff model). The EDS' characteristics collected included structural characteristics (location, type, size), daily workload (patients' number and severity, length of stay in hours), staff's participation (training, support to the intervention, leadership), type of week day (weekends vs weekdays) and time (in days). Associations between these variables and the staff model, the offer and acceptance rates were studied using multilevel modeling.
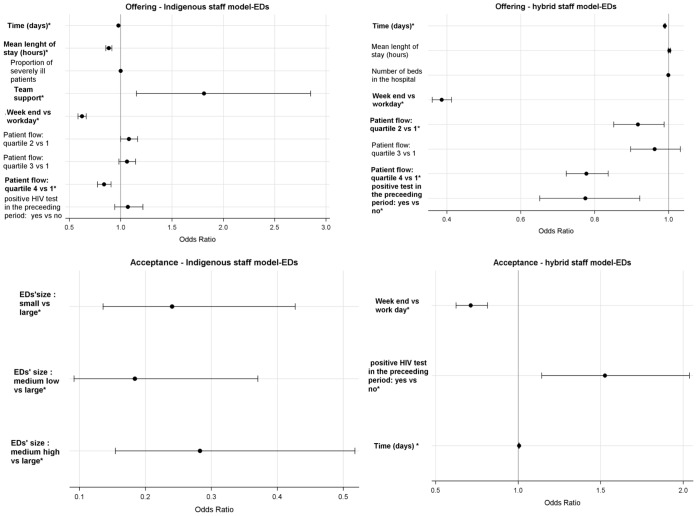
Results: Indigenous staff model was more frequent in EDs with a lower daily patient flow and a higher staff support score to the intervention. In indigenous-model EDs, the offer rate was associated with the patient flow (OR = 0.838, 95% CI = 0.773-0.908), was lower during weekends (OR = 0.623, 95% CI = 0.581-0.667) and decreased over time (OR = 0.978, 95% CI = 0.975-0.981). Similar results were found in hybrid-model EDs. Acceptance was poorly associated with EDs characteristics in indigenous-model EDs while in hybrid-model EDs it was lower during weekends (OR = 0.713, 95% CI = 0.623-0.816) and increased after the first positive test (OR = 1.526, 95% CI = 1.142-2.038). The EDs' characteristics explained respectively 38.5% and 15% of the total variance in the offer rate across indigenous model-EDs and hybrid model-EDs vs 12% and 1% for the acceptance rate.
Conclusion: Our findings suggest the need for taking into account EDs' characteristics while considering the implementation of an ED-based HIV screening program. Strategies allowing the optimization of human resources' utilization such as HIV targeted screening in the EDs might be privileged.
Conflict of interest statement
Figures
References
-
- Pitts SR, Niska RW, Xu J, Burt CW (2008) National Hospital Ambulatory Medical Care Survey: 2006 emergency department summary. Natl Health Stat Report: 1–38. - PubMed
-
- Direction de la Recherche, des Etudes, de l’Evaluation et des Statistiques (2006) L’activité des services d’urgences en 2004, une stabilisation du nombre de passages. Etudes et Résultats: 1–8.
-
- Rhodes KV, Gordon JA, Lowe RA (2000) Preventive care in the emergency department, Part I: Clinical preventive services–are they relevant to emergency medicine? Society for Academic Emergency Medicine Public Health and Education Task Force Preventive Services Work Group. Acad Emerg Med 7: 1036–1041. - PubMed
-
- Babcock Irvin C, Wyer PC, Gerson LW (2000) Preventive care in the emergency department, Part II: Clinical preventive services–an emergency medicine evidence-based review. Society for Academic Emergency Medicine Public Health and Education Task Force Preventive Services Work Group. Acad Emerg Med 7: 1042–1054. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
