

Factors associated with survival for patients with glioblastoma with poor pre-operative functional status
- PMID: 23639620
- PMCID: PMC3994533
- DOI: 10.1016/j.jocn.2012.07.016
Factors associated with survival for patients with glioblastoma with poor pre-operative functional status
Abstract
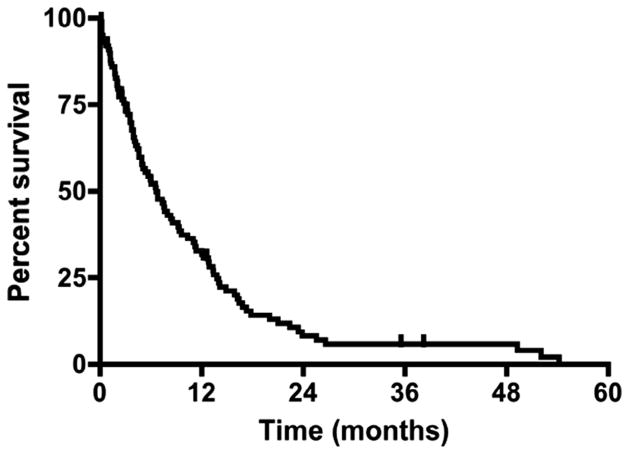
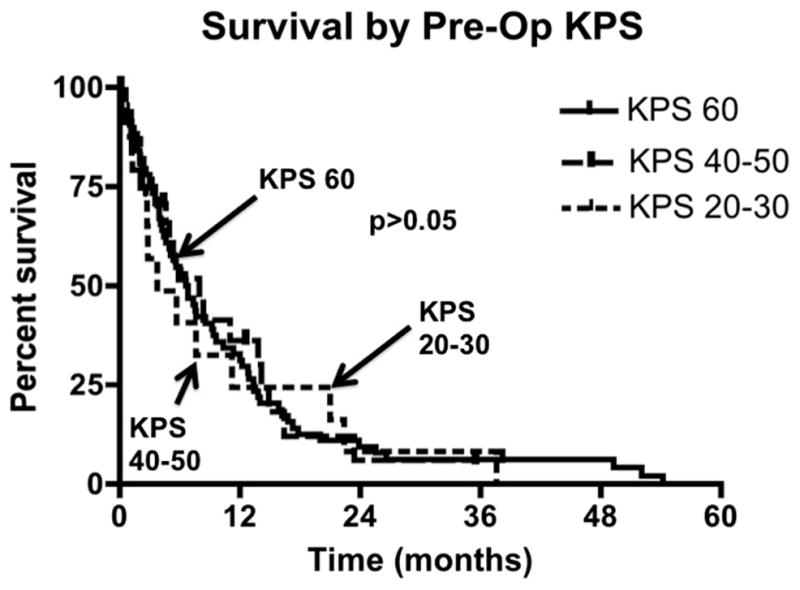
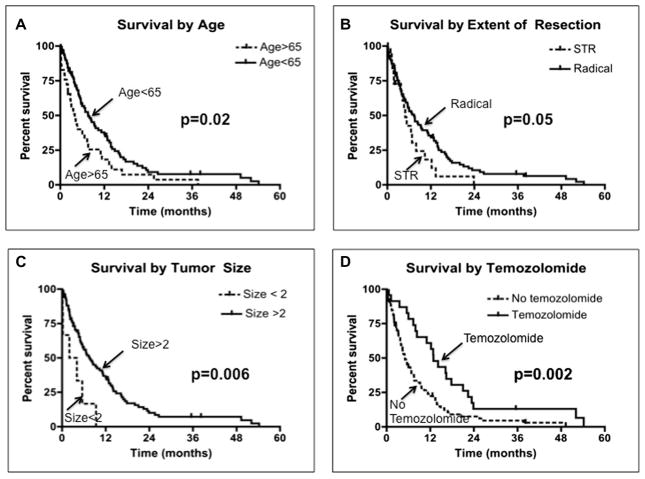
Patients with glioblastoma (GB) are known to have poor prognoses, and among these patients, those with poor neurological function have an even poorer prognosis. Consequently, aggressive surgeries and adjuvant therapies are often withheld because of this dismal outlook. The effects of aggressive therapies in this small subset of patients remain unknown. The goal of this study was to evaluate outcomes and factors associated with survival for poor functioning patients who underwent aggressive resection of their GB. Adult patients who underwent surgical resection of an intracranial primary GB at an academic tertiary-care institution between 1997 and 2007 were retrospectively reviewed. Patients with a Karnofsky Performance Scale (KPS) score of ≤60 were included. A total of 100 patients with primary GB met the inclusion criteria. The average age (± standard deviation) and KPS score of this cohort were 54 ± 15 years and 53 ± 12, respectively. No patient (0%) experienced perioperative mortality, and 0 (0%), 10 (10%), and 3 (3%) of patients incurred a new or increasing language, motor, and visual deficit, respectively. At last follow-up, 88 (88%) patients died with a median survival of 6.6 months. The factors associated with improved survival were age <65 year (p = 0.005), tumor size >2 cm (p = 0.01), radical tumor resection (p=0.01), and temozolomide (p = 0.001). This study identifies a subset of patients with poor functional status who may benefit from aggressive surgical resection.
Copyright © 2012 Elsevier Ltd. All rights reserved.
Conflict of interest statement
The authors declare that they have no financial or other conflicts of interest in relation to this research and its publication.
Figures
References
-
- Buckner JC. Factors influencing survival in high-grade gliomas. Semin Oncol. 2003;30:10–4. - PubMed
-
- Chaichana K, Parker S, Olivi A, et al. A proposed classification system that projects outcomes based on preoperative variables for adult patients with glioblastoma multiforme. J Neurosurg. 2010;112:997–1004. - PubMed
-
- DeAngelis LM. Brain tumors. N Engl J Med. 2001;344:114–23. - PubMed
-
- Lacroix M, Abi-Said D, Fourney DR, et al. A multivariate analysis of 416 patients with glioblastoma multiforme: prognosis, extent of resection, and survival. J Neurosurg. 2001;95:190–8. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
