

Underutilization of Lynch syndrome screening in a multisite study of patients with colorectal cancer
- PMID: 23639899
- PMCID: PMC3855589
- DOI: 10.1038/gim.2013.43
Underutilization of Lynch syndrome screening in a multisite study of patients with colorectal cancer
Abstract
Purpose: The aim of this study was to examine Lynch syndrome screening of patients with metastatic colorectal cancer in integrated health-care-delivery organizations.
Methods: We determined the availability of Lynch syndrome screening criteria and actual Lynch syndrome screening in the medical records of 1,188 patients diagnosed with metastatic colorectal cancer between 2004 and 2009 at seven institutions in the Cancer Research Network.
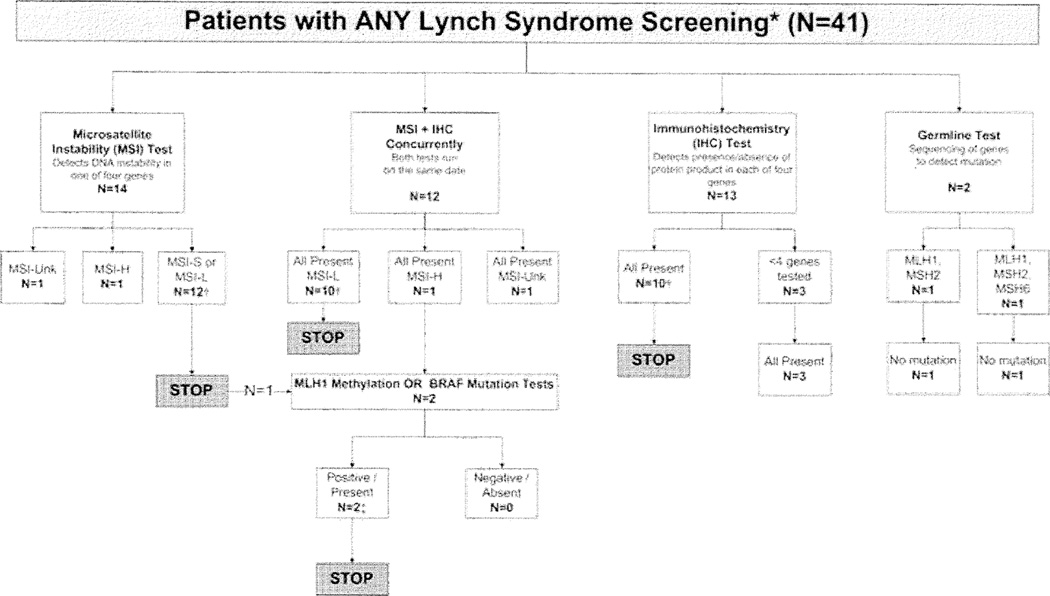
Results: We found infrequent use of Lynch syndrome screening (41/1,188). Family history was available for 937 of the 1,188 patients (79%). There was sufficient information to assess Lynch syndrome risk using family history-based criteria in 719 of the 937 patients (77%) with family history documentation. In 391 individuals with a family history of a Lynch syndrome-associated cancer, 107 (27%) could not be evaluated due to missing information such as age of cancer onset. Eleven percent of patients who met the Bethesda criteria and 25% of individuals who met the Amsterdam II criteria were screened for Lynch syndrome. Recommended guidelines were adhered to during screening, but no testing method was preferred.
Conclusion: The information required for Lynch syndrome screening decisions is routinely collected but seldom used. There is a critical gap between collection of family history and its use to guide Lynch syndrome screening, which may support a case for implementation of universal screening guidelines.
Conflict of interest statement
Figures

References
-
- American Cancer Society. [Accessed July 29, 2012];Cancer Facts & Figures 2012. 2012 http://www.cancer.org/acs/groups/content/@epidemiologysurveilance/docume.... accessed 08/07/2012.
-
- U.S. Cancer Statistics Working Group. U.S. Department of Health and Human Services, Centers for Disesae Control and Prevention, National Cancer Institute. [accessed December 19, 2012];United States Cancer Statistics: 1999–2008 incidence and mortality web-based report, 2012 update. 2012 http://apps.nccd.cdc.gov/uscs.
-
- Hampel H, Frankel WL, Martin E, et al. Screening for the Lynch Syndrome (Hereditary Nonpolyposis Colorectal Cancer) N Engl J Med. 2005;352:1851–1860. - PubMed
-
- Lynch HT, de la Chapelle A. Hereditary colorectal cancer. N Engl J Med. 2003;348:919–932. - PubMed
-
- Weissman SM, Burt R, Church J, et al. Identification of individuals at risk for lynch syndrome using targeted evaluations and genetic testing: national society of genetic counselors and the collaborative group of the americas on inherited colorectal cancer joint practice guideline. J Genet Couns. 2012;21:484–493. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
