

Tuberculosis: From an incurable scourge to a curable disease - journey over a millennium
- PMID: 23640554
- PMCID: PMC3705655
Tuberculosis: From an incurable scourge to a curable disease - journey over a millennium
Abstract
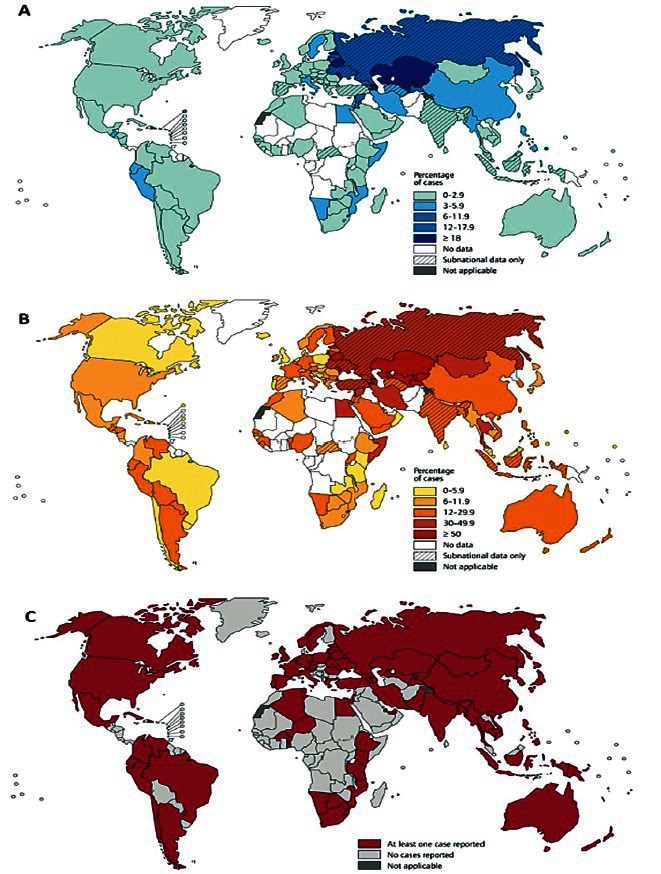
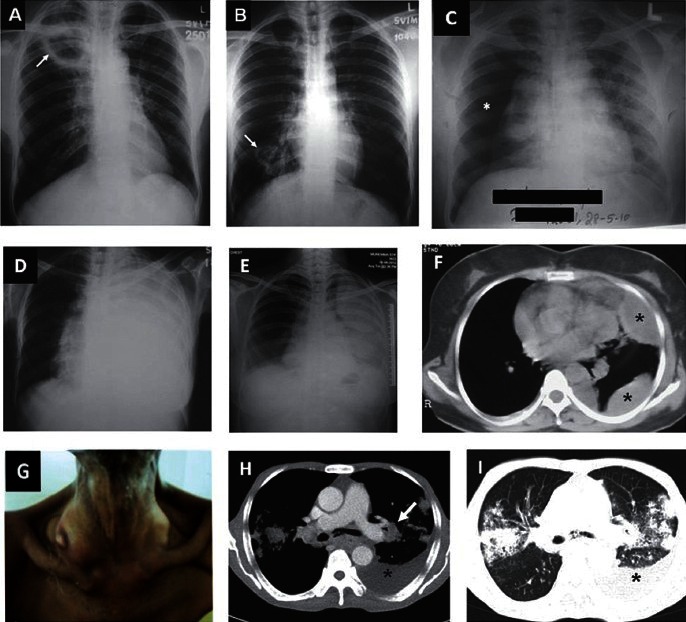
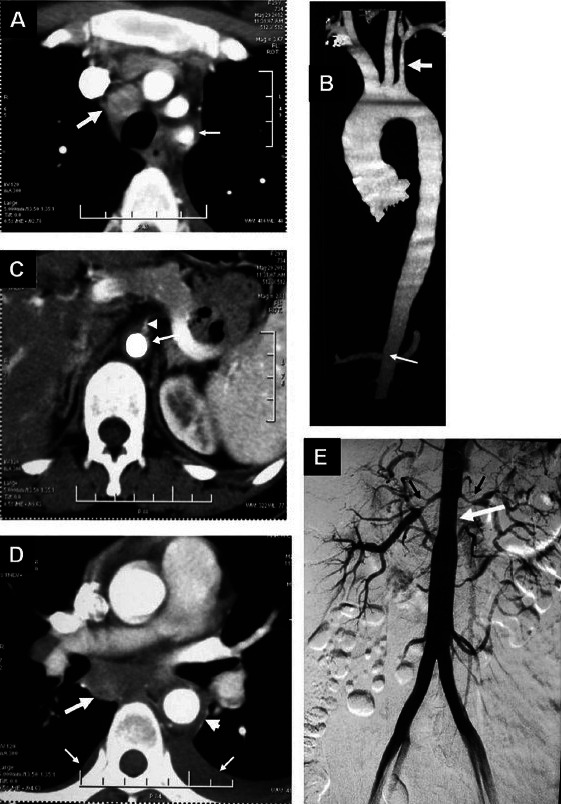
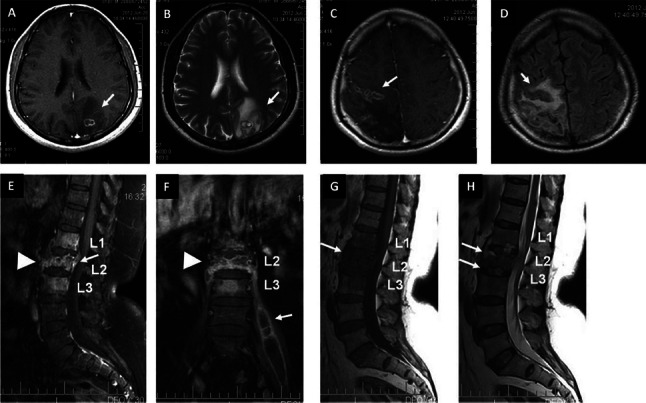
Globally, tuberculosis (TB) still remains a major public health problem. India is a high TB burden country contributing to 26 per cent of global TB burden. During 1944-1980, TB became treatable and short-course chemotherapy emerged as the standard of care. When TB elimination seemed possible in the early 1980s, global human immunodeficiency virus (HIV) infection/acquired immunodeficiency syndrome (AIDS) pandemic resulted in a resurgence of TB. Widespread occurrence of multidrug-resistant and extensively drug-resistant TB (M/XDR-TB) is threatening to destabilize TB control globally. Atypical clinical presentation still poses a challenge. Disseminated, miliary and cryptic TB are being increasingly recognized. Availability of newer imaging modalities has allowed more efficient localization of lesions and use of image guided procedures has facilitated definitive diagnosis of extrapulmonary TB. Introduction of liquid culture, rapid drug-susceptibility testing (DST), molecular diagnostic methods has helped in rapid detection, speciation and DST profiling of Mycobacterium tuberculosis isolates. While treatment of TB and HIV-TB co-infection has become simpler, efforts are on to shorten the treatment duration. However, drug toxicities and drug-drug interactions still constitute a significant challenge. Recently, there has been better understanding of anti-TB drug-induced hepatotoxicity and its frequent confounding by viral hepatitis, especially, in resource-constrained settings; and immune reconstitution inflammatory syndrome (IRIS) in HIV-TB. Quest for newer biomarkers for predicting a durable cure, relapse, discovery/repurposing of newer anti-TB drugs, development of newer vaccines continues to achieve the goal of eliminating TB altogether by 2050.
Figures



References
-
- Mohan A, Sharma SK. History. In: Sharma SK, Mohan A, editors. Tuberculosis. 2nd ed. New Delhi: Jaypee Brothers Medical Publishers; 2009. pp. 7–15.
-
- Rubin SA. Tuberculosis. Captain of all these men of death. Radiol Clin North Am. 1995;33:619–39. - PubMed
-
- Dubos R, Dubos J. Boston: Little, Brown and Company; 1952. The white plague. Tuberculosis, man and society.
-
- Waksman SA. Berkeley and Los Angeles: University of California Press; 1964. The conquest of tuberculosis.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical