

Renal ischemia-reperfusion injury amplifies the humoral immune response
- PMID: 23641055
- PMCID: PMC3699821
- DOI: 10.1681/ASN.2012060560
Renal ischemia-reperfusion injury amplifies the humoral immune response
Abstract
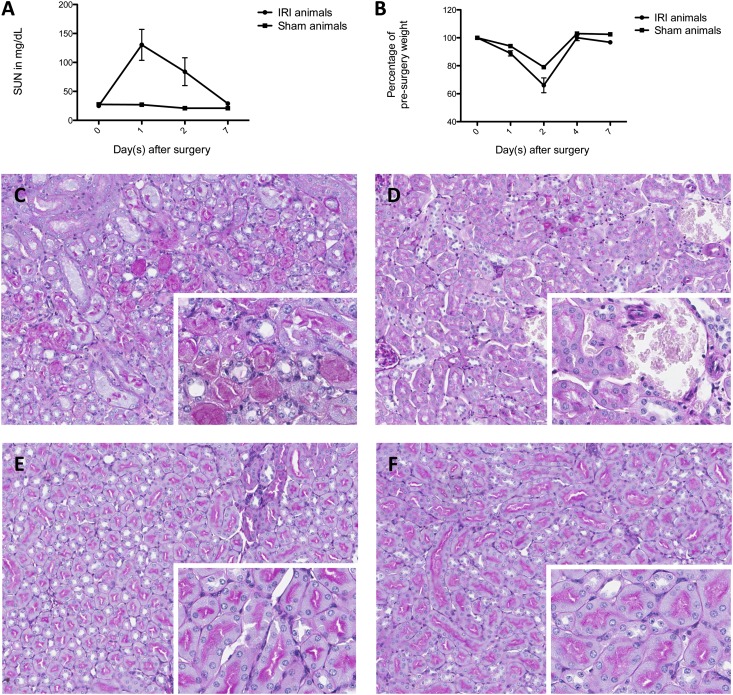
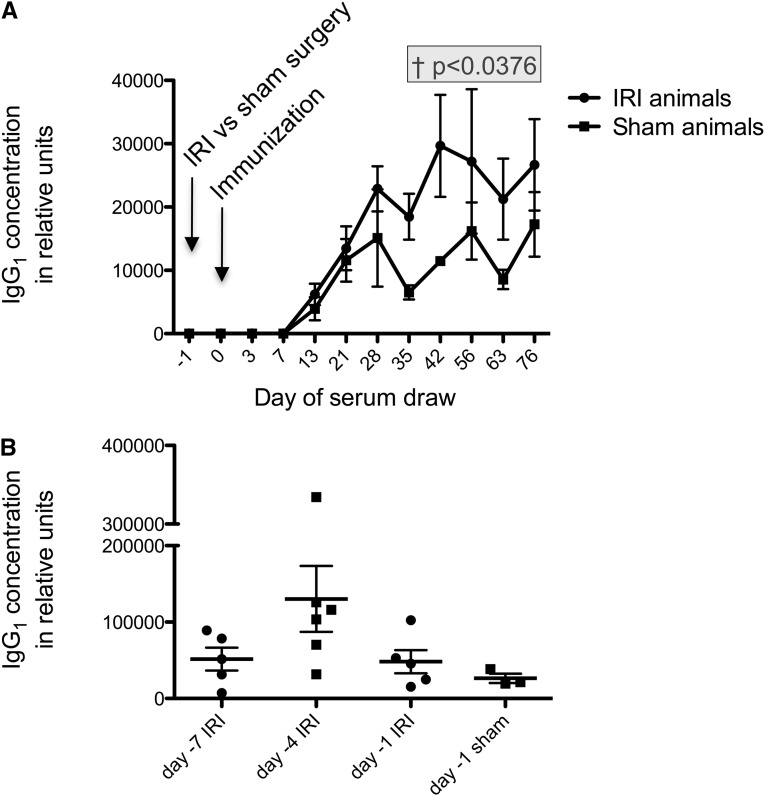
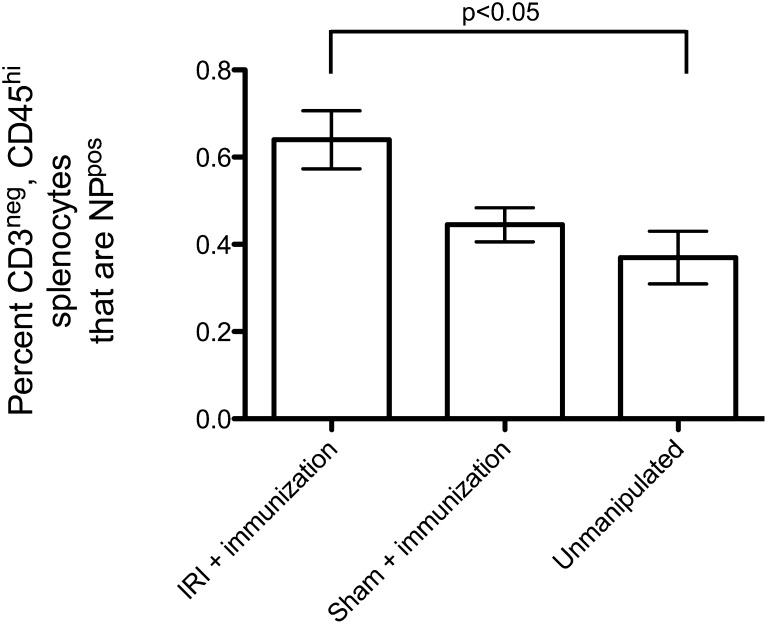
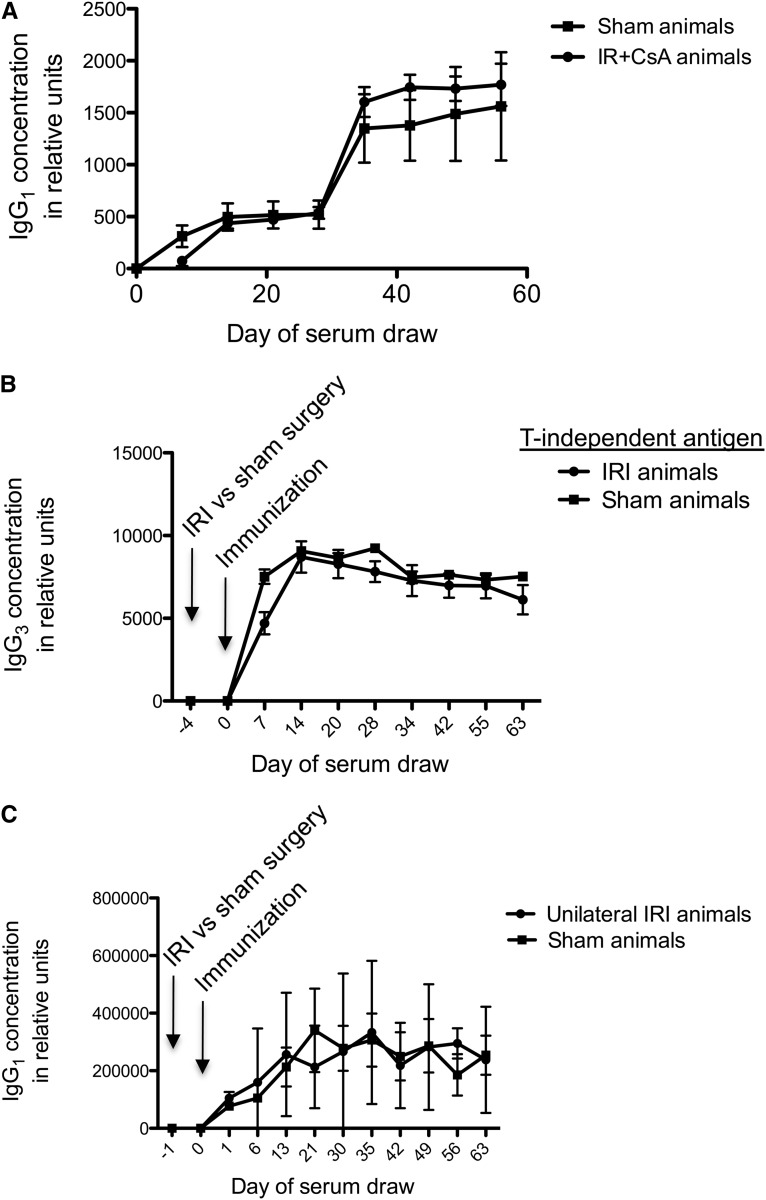
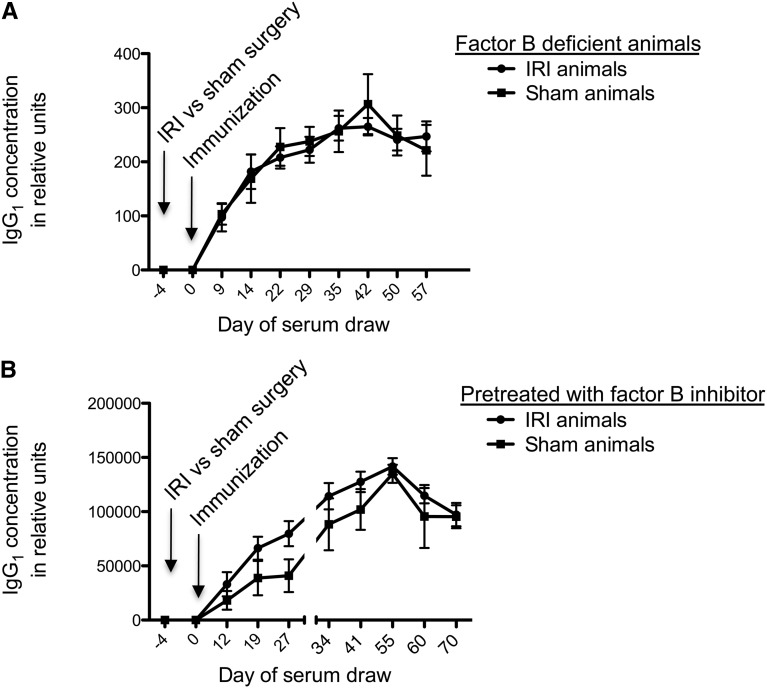
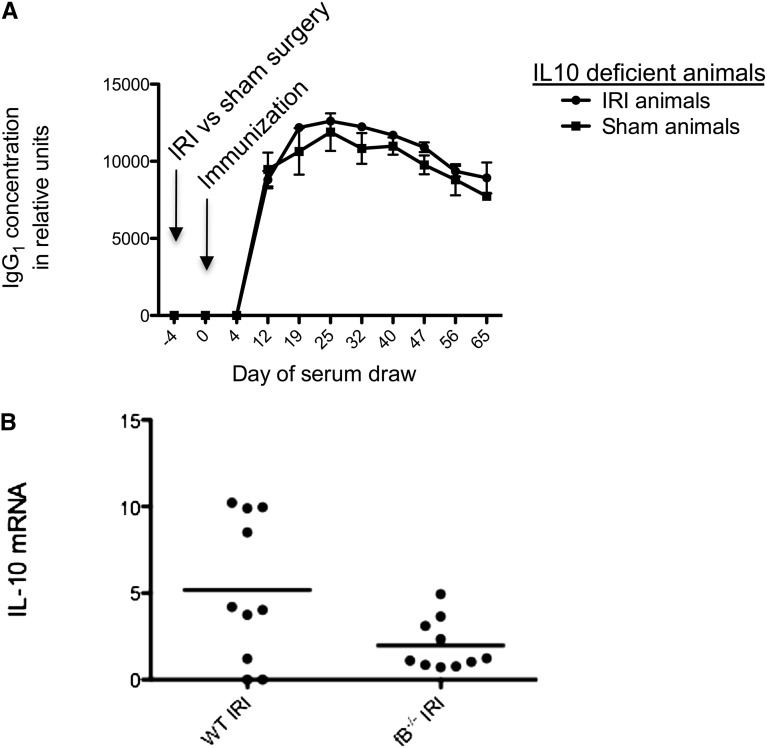
Renal transplant recipients who experience delayed graft function have increased risks of rejection and long-term graft failure. Ischemic damage is the most common cause of delayed graft function, and although it is known that tissue inflammation accompanies renal ischemia, it is unknown whether renal ischemia affects the production of antibodies by B lymphocytes, which may lead to chronic humoral rejection and allograft failure. Here, mice immunized with a foreign antigen 24-96 hours after renal ischemia-reperfusion injury developed increased levels of antigen-specific IgG1 compared with sham-treated controls. This amplified IgG1 response did not follow unilateral ischemia, and it did not occur in response to a T-independent antigen. To test whether innate immune activation in the kidney after ischemia affects the systemic immune response to antigen, we repeated the immunization experiment using mice deficient in factor B that lack a functional alternative pathway of complement. Renal ischemia-reperfusion injury did not cause amplification of the antigen-specific antibodies in these mice, suggesting that the increased immune response requires a functional alternative pathway of complement. Taken together, these data suggest that ischemic renal injury leads to a rise in antibody production, which may be harmful to renal allografts, possibly explaining a mechanism underlying the link between delayed graft function and long-term allograft failure.
Figures
References
-
- Quiroga I, McShane P, Koo DD, Gray D, Friend PJ, Fuggle S, Darby C: Major effects of delayed graft function and cold ischaemia time on renal allograft survival. Nephrol Dial Transplant 21: 1689–1696, 2006 - PubMed
-
- Ojo AO, Wolfe RA, Held PJ, Port FK, Schmouder RL: Delayed graft function: Risk factors and implications for renal allograft survival. Transplantation 63: 968–974, 1997 - PubMed
-
- Nogueira JM, Haririan A, Jacobs SC, Weir MR, Hurley HA, Al-Qudah HS, Phelan M, Drachenberg CB, Bartlett ST, Cooper M: The detrimental effect of poor early graft function after laparoscopic live donor nephrectomy on graft outcomes. Am J Transplant 9: 337–347, 2009 - PubMed
-
- Narayanan R, Cardella CJ, Cattran DC, Cole EH, Tinckam KJ, Schiff J, Kim SJ: Delayed graft function and the risk of death with graft function in living donor kidney transplant recipients. Am J Kidney Dis 56: 961–970, 2010 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
