

IBCD: development and testing of a checklist to improve quality of care for hospitalized general medical patients
- PMID: 23641534
- PMCID: PMC4005500
- DOI: 10.1016/s1553-7250(13)39021-7
IBCD: development and testing of a checklist to improve quality of care for hospitalized general medical patients
Abstract
Background: Several studies have demonstrated the usefulness of medical checklists to improve quality of care in surgery and the ICU. The feasibility, effectiveness, and sustainability of a checklist was explored.
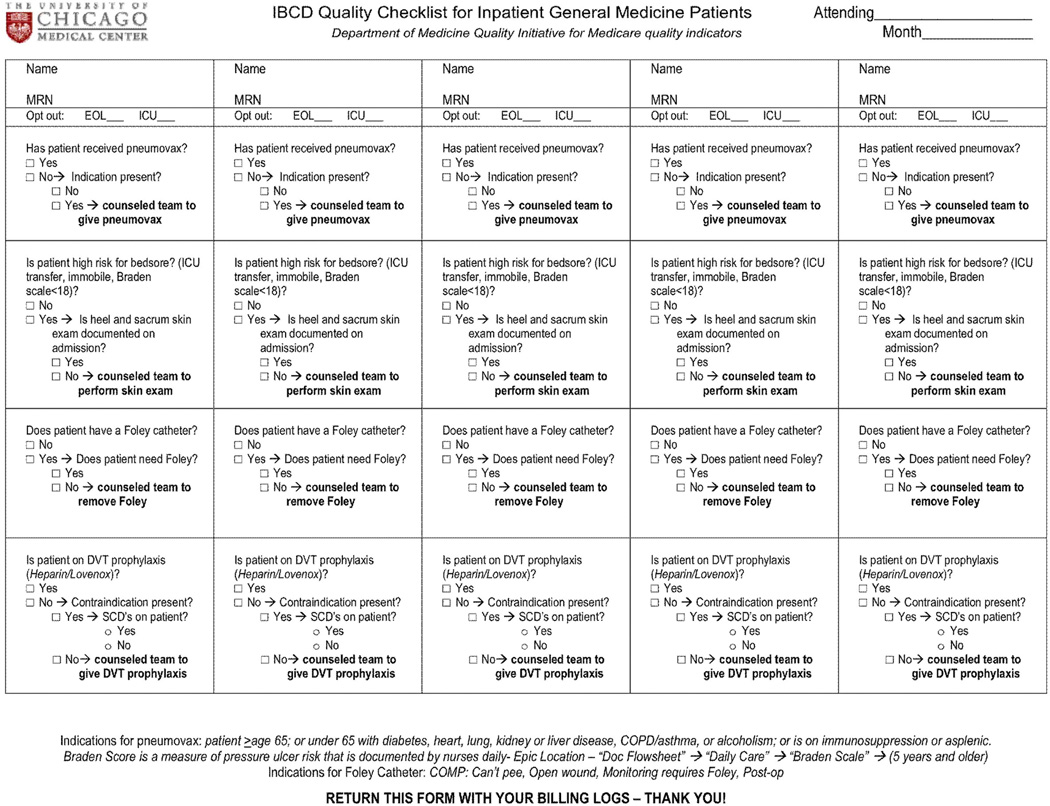
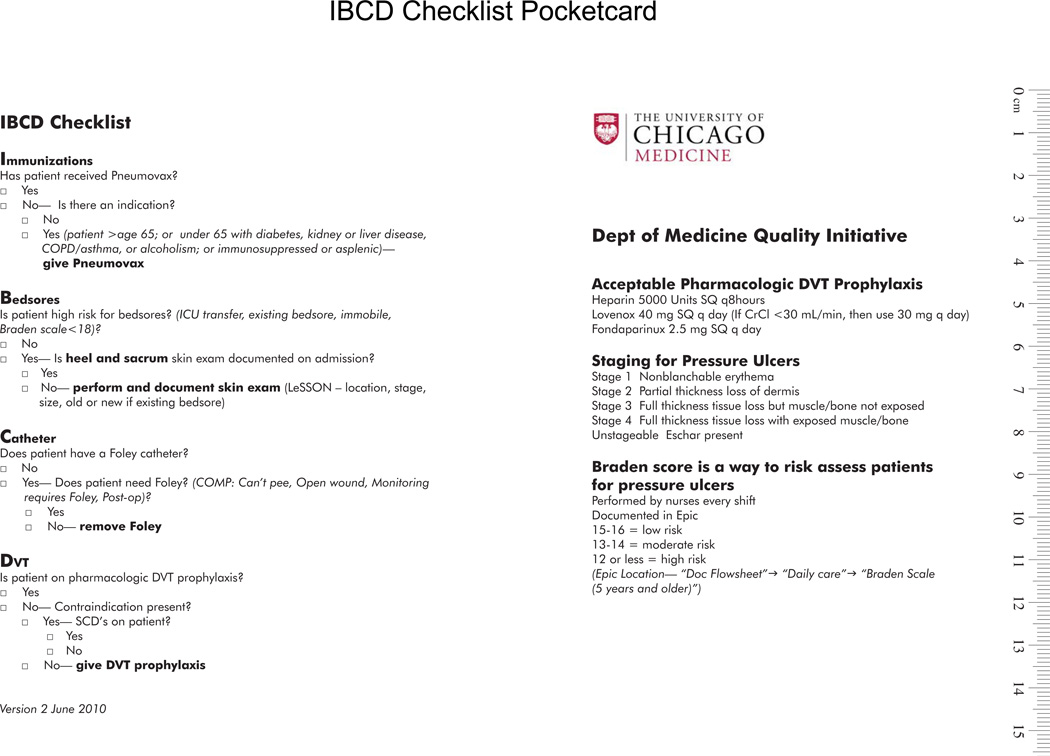
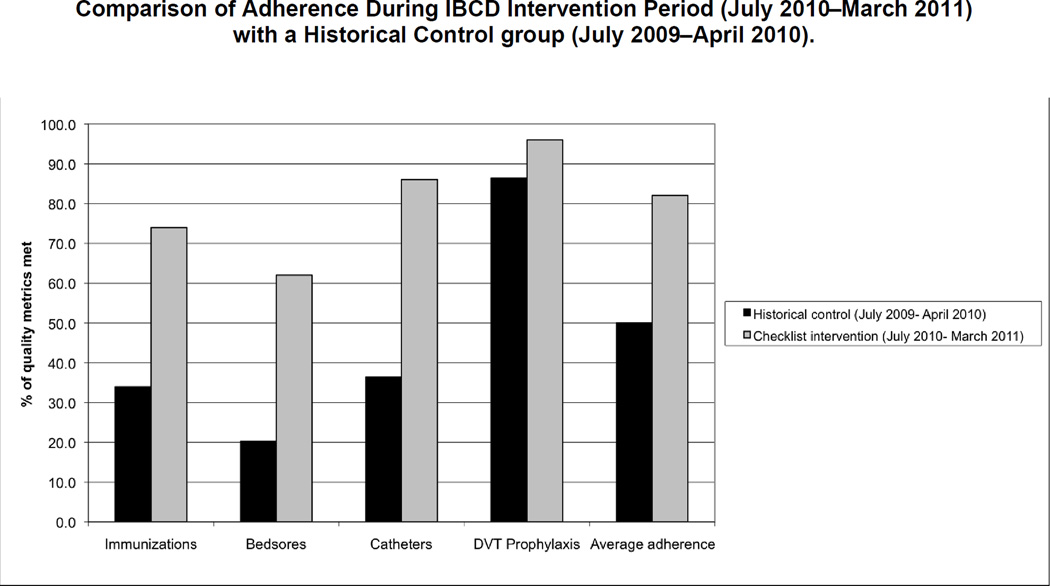
Methods: Literature on checklists and adherence to quality indicators in general medicine was reviewed to develop evidence-based measures for the IBCD checklist: (I) pneumococcal immunization, (B) pressure ulcers (bedsores), (C) catheter-associated urinary tract infections (CAUTIs), and (D) deep venous thrombosis (DVT) were considered conditions highly relevant to the quality of care in general medicine inpatients. The checklist was used by attending physicians during rounds to remind residents to perform four actions related to these measures. Charts were audited to document actions prompted by the checklist.
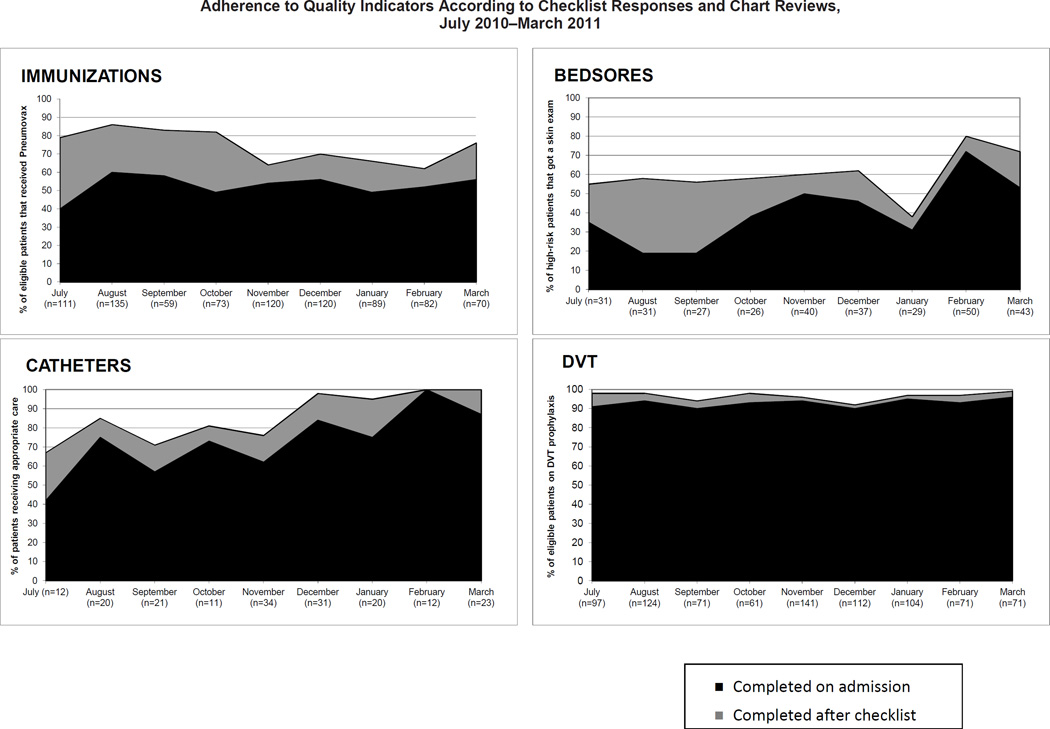
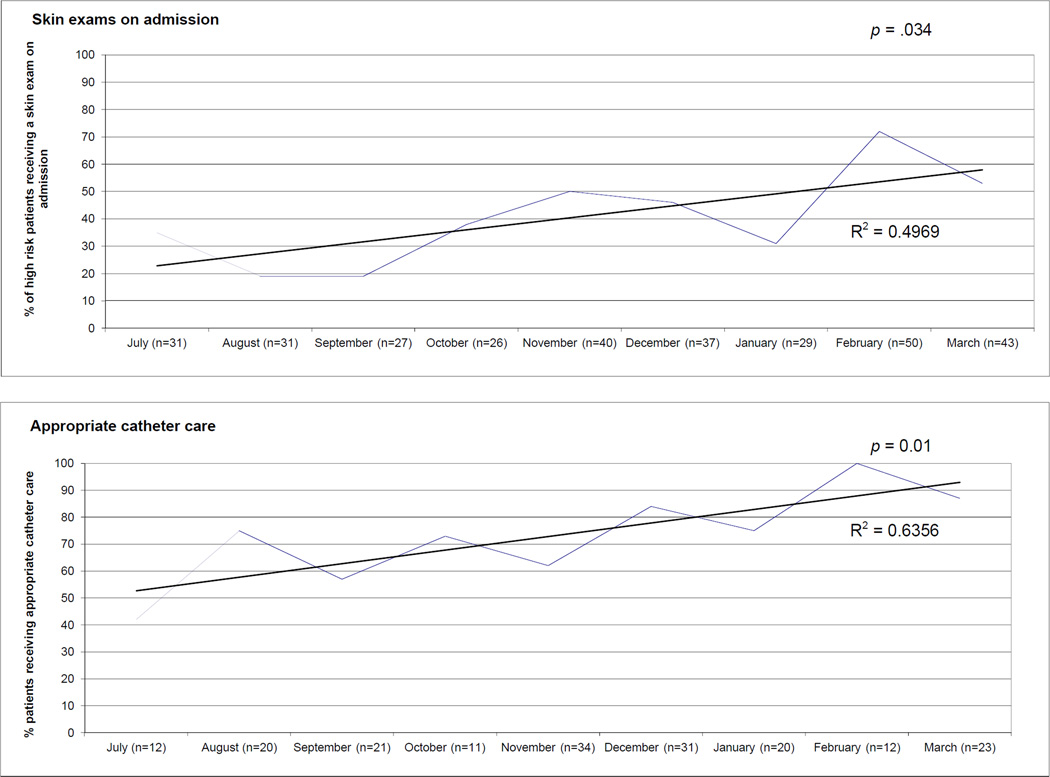
Results: The IBCD checklist was associated with significantly increased documentation of and adherence to care processes associated with these four quality indicators. Seventy percent (46/66) of general medicine teams during the intervention period of July 2010-March 2011 voluntarily used the IBCD checklist for 1,168 (54%) of 2,161 patients. During the intervention period, average adherence for all four checklist items increased from 68% on admission to 82% after checklist use (p < .001). Average adherence after checklist use was also higher when compared to a historical control group from one year before implementation (82% versus 50%, p < .0001). In the six weeks after the checklist was transitioned to the electronic medical record, IBCD was noted in documentation of 133 (59%) of 226 patients admitted to general medicine.
Conclusion: A checklist is a useful and sustainable tool to improve adherence to, and documentation of, care processes specific to quality indicators in general medicine.
Figures
References
-
- Davidoff F. Checklists and guidelines: Imaging techniques for visualizing what to do. JAMA. 2010 Jul 4;304(2):206–207. - PubMed
-
- Hales BM, Pronovost PJ. The checklist: A tool for error management and performance improvement. J Crit Care. 2006;21(3):231–235. - PubMed
-
- Gawande A. The Checklist Manifesto. New York City: Metropolitan Books; 2009.
-
- Pronovost P. Interventions to decrease catheter-related bloodstream infections in the ICU: The keystone intensive care unit project. Am J Infect Control. 2008;36(10):S171, e1–e5. - PubMed
-
- Haynes AB, et al. Safe Surgery Saves Lives Study Group. A surgical safety checklist to reduce morbidity and mortality in a global population. N Engl J Med. 2009 Jan 29;360(5):491–499. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
