

A solitary hyperfunctioning thyroid nodule harboring thyroid carcinoma: review of the literature
- PMID: 23641736
- PMCID: PMC3655919
- DOI: 10.1186/1756-6614-6-7
A solitary hyperfunctioning thyroid nodule harboring thyroid carcinoma: review of the literature
Abstract
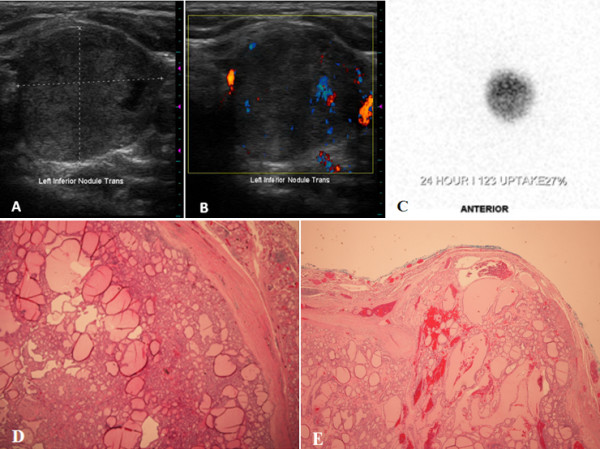
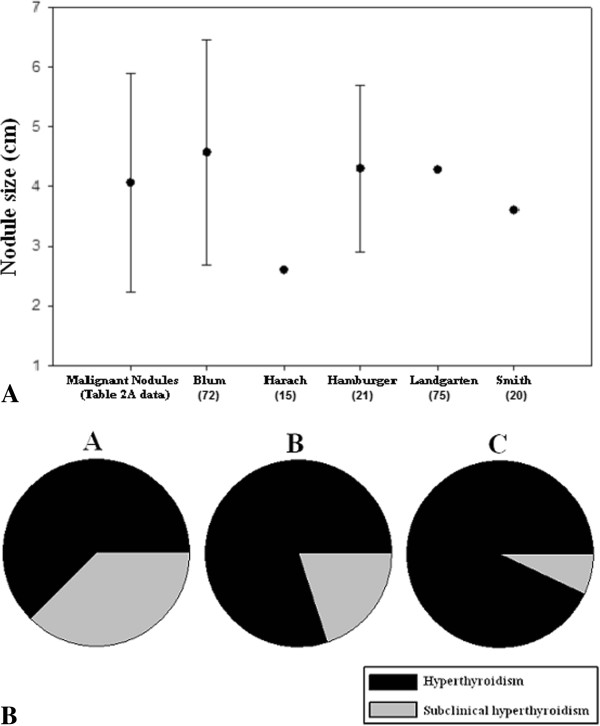
Hyperfunctioning nodules of the thyroid are thought to only rarely harbor thyroid cancer, and thus are infrequently biopsied. Here, we present the case of a patient with a hyperfunctioning thyroid nodule harboring thyroid carcinoma and, using MEDLINE literature searches, set out to determine the prevalence of and characteristics of malignant "hot" nodules as a group. Historical, biochemical and radiologic characteristics of the case subjects and their nodules were compared to those in cases of benign hyperfunctioning nodules. A literature review of surgical patients with solitary hyperfunctioning thyroid nodules managed by thyroid resection revealed an estimated 3.1% prevalence of malignancy. A separate literature search uncovered 76 cases of reported malignant hot thyroid nodules, besides the present case. Of these, 78% were female and mean age at time of diagnosis was 47 years. Mean nodule size was 4.13 ± 1.68 cm. Laboratory assessment revealed T3 elevation in 76.5%, T4 elevation in 51.9%, and subclinical hyperthyroidism in 13% of patients. Histological diagnosis was papillary thyroid carcinoma (PTC) in 57.1%, follicular thyroid carcinoma (FTC) in 36.4%, and Hurthle cell carcinoma in 7.8% of patients. Thus, hot thyroid nodules harbor a low but non-trivial rate of malignancy. Compared to individuals with benign hyperfunctioning thyroid nodules, those with malignant hyperfunctioning nodules are younger and more predominantly female. Also, FTC and Hurthle cell carcinoma are found more frequently in hot nodules than in general. We were unable to find any specific characteristics that could be used to distinguish between malignant and benign hot nodules.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
