

Wave intensity analysis in the human coronary circulation in health and disease
- PMID: 23642024
- PMCID: PMC3968589
- DOI: 10.2174/1573403x10999140226121300
Wave intensity analysis in the human coronary circulation in health and disease
Abstract
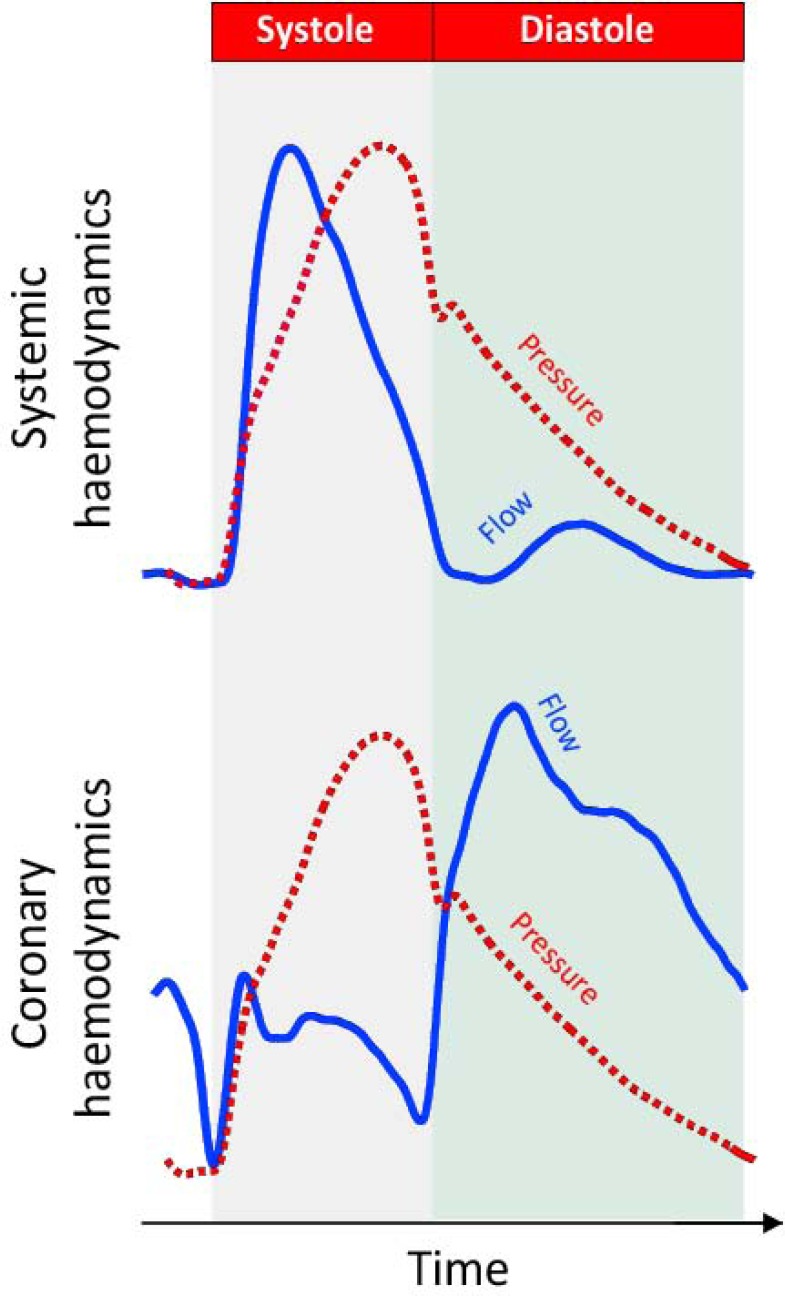
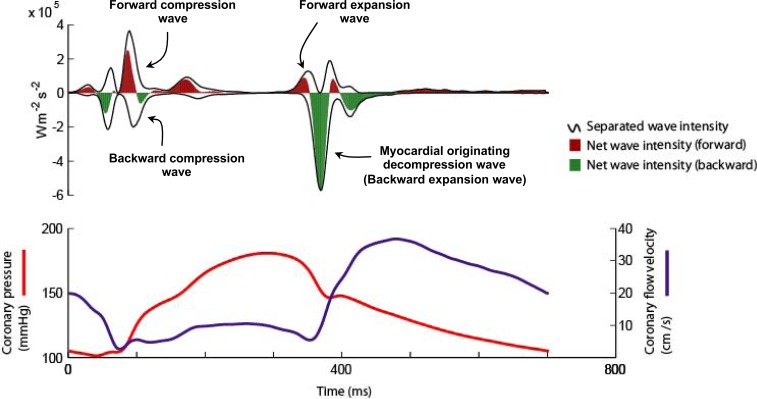
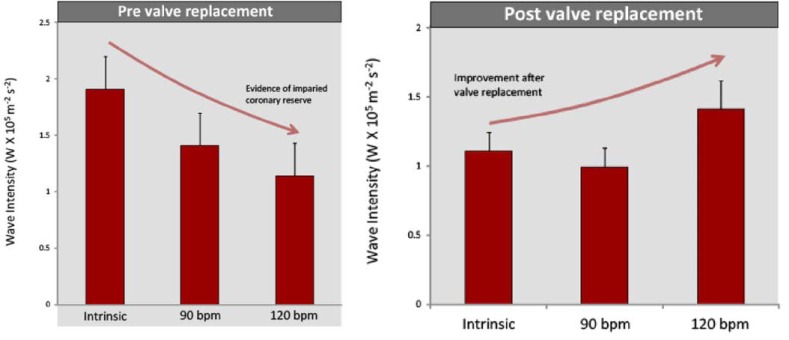
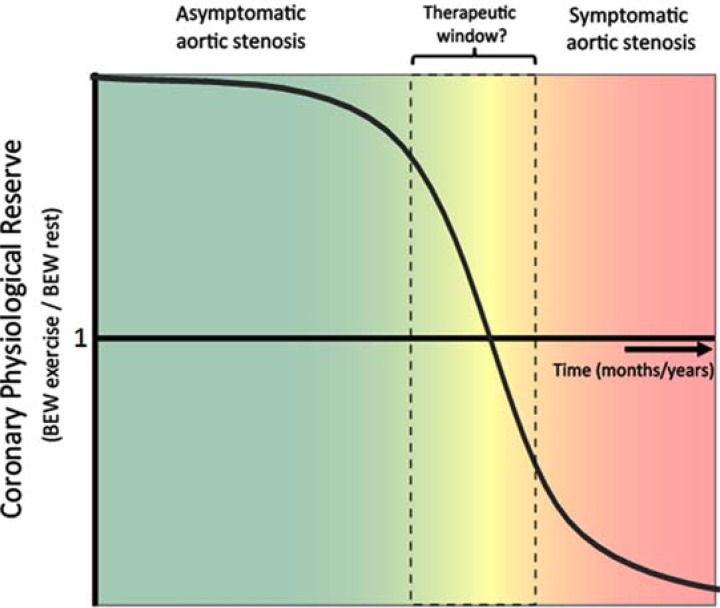
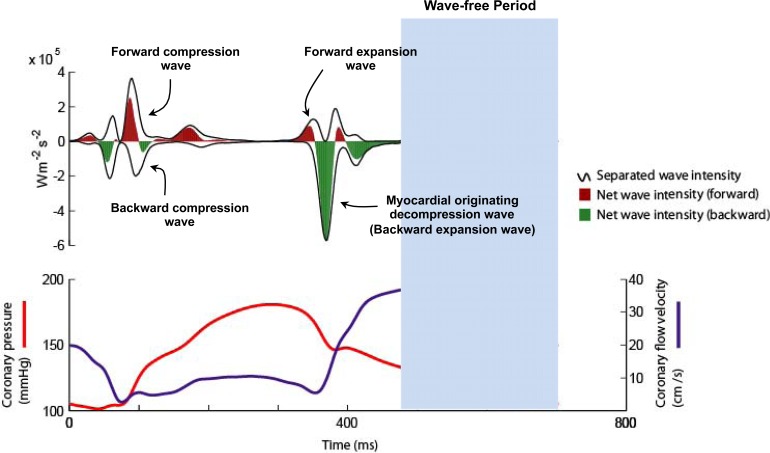
Coronary artery hemodynamics are very different to that of the systemic arteries; unlike the systemic circulation, in the coronary circulation pressure is generated from both the proximal and distal end of the artery - due to the effect of contraction and relaxation of the myocardium on the microvasculature. As a result, the systemic artery hemodynamic model cannot be used to explain the pressure-flow relationship in the coronaries. Wave intensity analysis is an investigative tool that is able to distinguish simultaneous proximal and distal influences on coronary blood flow and is therefore uniquely suitable for the study of coronary haemodynamics. This review discusses the concept behind wave intensity analysis and evaluates how it has been used to characterise and provide new insights on coronary haemodynamics in health and disease.
Figures
Similar articles
-
Arterial wave intensity and ventriculoarterial interaction.Heart Vessels. 1997;Suppl 12:128-34. Heart Vessels. 1997. PMID: 9476563 Review.
-
Intramyocardial influences on blood flow distributions in the myocardial wall.Ann Biomed Eng. 2000 Aug;28(8):897-902. doi: 10.1114/1.1308487. Ann Biomed Eng. 2000. PMID: 11144673 Review.
-
Coronary blood flow changes during atrioventricular sequential pacing with different atrioventricular delays in normal individuals.J Interv Card Electrophysiol. 1998 Jun;2(2):163-9. doi: 10.1023/a:1009703632271. J Interv Card Electrophysiol. 1998. PMID: 9870008
-
Differences in cardiac microcirculatory wave patterns between the proximal left mainstem and proximal right coronary artery.Am J Physiol Heart Circ Physiol. 2008 Sep;295(3):H1198-H1205. doi: 10.1152/ajpheart.00510.2008. Epub 2008 Jul 18. Am J Physiol Heart Circ Physiol. 2008. PMID: 18641272 Free PMC article.
-
The coronary circulation: quo vadis?Cardiologia. 1999 Aug;44(8):699-710. Cardiologia. 1999. PMID: 10476595 Review.
Cited by
-
Primary versus iatrogenic (post-PCI) coronary microvascular dysfunction: a wire-based multimodal comparison.Open Heart. 2023 Nov 27;10(2):e002437. doi: 10.1136/openhrt-2023-002437. Open Heart. 2023. PMID: 38011991 Free PMC article. Clinical Trial.
-
Microcirculatory Disease in Patients after Heart Transplantation.J Clin Med. 2023 Jun 4;12(11):3838. doi: 10.3390/jcm12113838. J Clin Med. 2023. PMID: 37298033 Free PMC article. Review.
-
Assessing Coronary Blood Flow Physiology in the Cardiac Catheterisation Laboratory.Curr Cardiol Rev. 2017;13(3):232-243. doi: 10.2174/1573403X13666170525102618. Curr Cardiol Rev. 2017. PMID: 28545351 Free PMC article. Review.
-
Impact of coronary bifurcation morphology on wave propagation.Am J Physiol Heart Circ Physiol. 2016 Oct 1;311(4):H855-H870. doi: 10.1152/ajpheart.00130.2016. Epub 2016 Jul 8. Am J Physiol Heart Circ Physiol. 2016. PMID: 27402665 Free PMC article.
-
LDL‑induced NLRC3 inflammasome activation in cardiac fibroblasts contributes to cardiomyocytic dysfunction.Mol Med Rep. 2021 Jul;24(1):526. doi: 10.3892/mmr.2021.12165. Epub 2021 May 26. Mol Med Rep. 2021. PMID: 34036387 Free PMC article.
References
-
- Davies JE, Whinnett ZI, Francis DP, et al. Evidence of a dominant backward-propagating "suction" wave responsible for diastolic coronary filling in humans attenuated in left ventricular hypertrophy. Circulation. 2006;113(14):1768–78. - PubMed
-
- Parker KH, Jones CJ. Forward and backward running waves in the arteries analysis using the method of characteristics. J Biomech Eng. 1990;112(3):322–6. - PubMed
-
- Parker KH. An introduction to wave intensity analysis. Med Biol Eng Comput. 2009;47(2):175–88. - PubMed
-
- Spaan JA, Breuls NP, Laird JD. Diastolic-systolic coronary flow differences are caused by intramyocardial pump action in the anesthetized dog. Circ Res. 1981;49(3):584–93. - PubMed
-
- Davies JE, Whinnett ZI, Francis DP, et al. Use of simultaneous pressure and velocity measurements to estimate arterial wave speed at a single site in humans. Am J Physiol Heart Circ Physiol. 2006;290(2):H878–85. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
