

Lupus enteritis: from clinical findings to therapeutic management
- PMID: 23642042
- PMCID: PMC3651279
- DOI: 10.1186/1750-1172-8-67
Lupus enteritis: from clinical findings to therapeutic management
Abstract
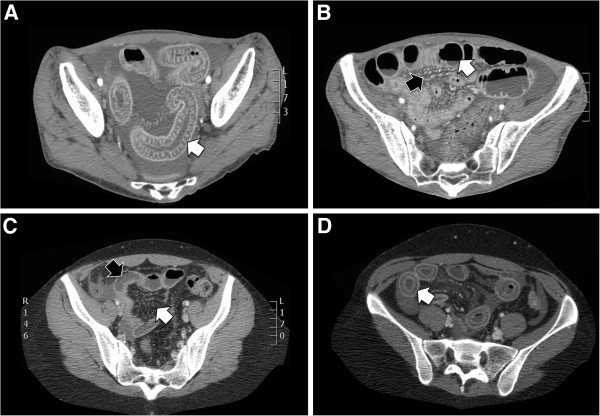
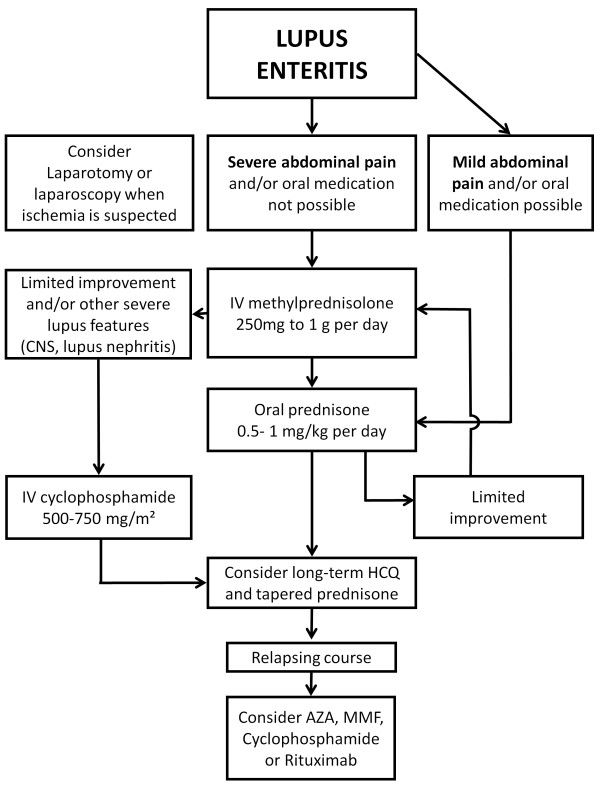
Lupus enteritis is a rare and poorly understood cause of abdominal pain in patients with systemic lupus erythematosus (SLE). In this study, we report a series of 7 new patients with this rare condition who were referred to French tertiary care centers and perform a systematic literature review of SLE cases fulfilling the revised ACR criteria, with evidence for small bowel involvement, excluding those with infectious enteritis. We describe the characteristics of 143 previously published and 7 new cases. Clinical symptoms mostly included abdominal pain (97%), vomiting (42%), diarrhea (32%) and fever (20%). Laboratory features mostly reflected lupus activity: low complement levels (88%), anemia (52%), leukocytopenia or lymphocytopenia (40%) and thrombocytopenia (21%). Median CRP level was 2.0 mg/dL (range 0-8.2 mg/dL). Proteinuria was present in 47% of cases. Imaging studies revealed bowel wall edema (95%), ascites (78%), the characteristic target sign (71%), mesenteric abnormalities (71%) and bowel dilatation (24%). Only 9 patients (6%) had histologically confirmed vasculitis. All patients received corticosteroids as a first-line therapy, with additional immunosuppressants administered either from the initial episode or only in case of relapse (recurrence rate: 25%). Seven percent developed intestinal necrosis or perforation, yielding a mortality rate of 2.7%. Altogether, lupus enteritis is a poorly known cause of abdominal pain in SLE patients, with distinct clinical and therapeutic features. The disease may evolve to intestinal necrosis and perforation if untreated. Adding with this an excellent steroid responsiveness, timely diagnosis becomes primordial for the adequate management of this rare entity.
Figures
References
-
- Cacoub P, Benhamou Y, Barbet P, Piette JC, Le Cae A, Chaussade S, Cadranel JF, Callard P, Opolon P, Godeau P. Systemic lupus erythematosus and chronic intestinal pseudoobstruction. J Rheumatol. 1993;20(2):377–381. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
