

Brittle cornea syndrome: recognition, molecular diagnosis and management
- PMID: 23642083
- PMCID: PMC3659006
- DOI: 10.1186/1750-1172-8-68
Brittle cornea syndrome: recognition, molecular diagnosis and management
Abstract
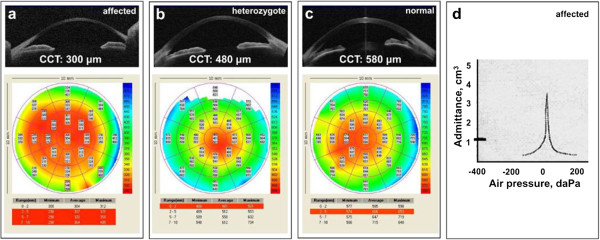
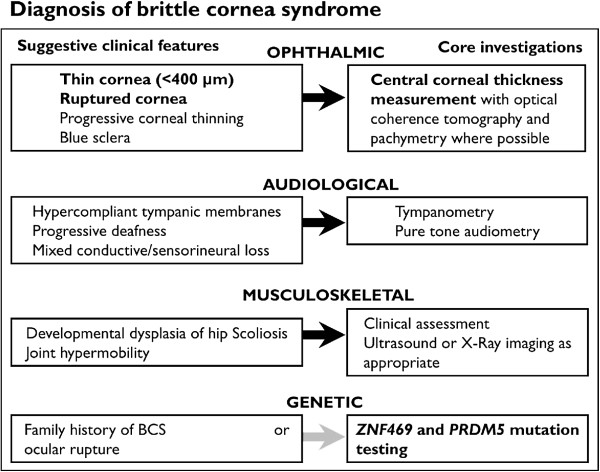
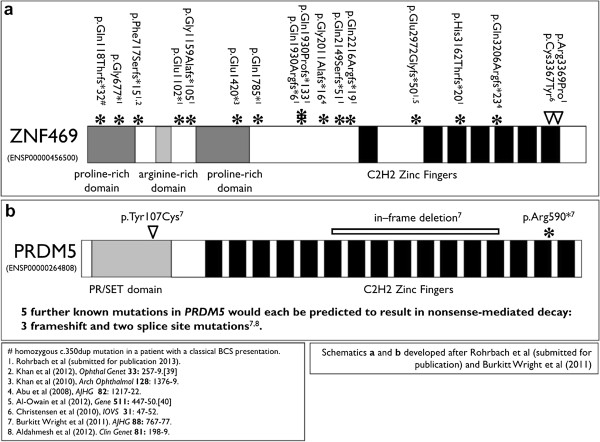
Brittle cornea syndrome (BCS) is an autosomal recessive disorder characterised by extreme corneal thinning and fragility. Corneal rupture can therefore occur either spontaneously or following minimal trauma in affected patients. Two genes, ZNF469 and PRDM5, have now been identified, in which causative pathogenic mutations collectively account for the condition in nearly all patients with BCS ascertained to date. Therefore, effective molecular diagnosis is now available for affected patients, and those at risk of being heterozygous carriers for BCS. We have previously identified mutations in ZNF469 in 14 families (in addition to 6 reported by others in the literature), and in PRDM5 in 8 families (with 1 further family now published by others). Clinical features include extreme corneal thinning with rupture, high myopia, blue sclerae, deafness of mixed aetiology with hypercompliant tympanic membranes, and variable skeletal manifestations. Corneal rupture may be the presenting feature of BCS, and it is possible that this may be incorrectly attributed to non-accidental injury. Mainstays of management include the prevention of ocular rupture by provision of protective polycarbonate spectacles, careful monitoring of visual and auditory function, and assessment for skeletal complications such as developmental dysplasia of the hip. Effective management depends upon appropriate identification of affected individuals, which may be challenging given the phenotypic overlap of BCS with other connective tissue disorders.
Figures

References
-
- Burkitt Wright EM, Spencer HL, Daly SB, Manson FD, Zeef LA, Urquhart J, Zoppi N, Bonshek R, Tosounidis I, Mohan M, Madden C, Dodds A, Chandler KE, Banka S, Au L, Clayton-Smith J, Khan N, Biesecker LG, Wilson M, Rohrbach M, Colombi M, Giunta C, Black GC. Mutations in PRDM5 in brittle cornea syndrome identify a pathway regulating extracellular matrix development and maintenance. Am J Hum Genet. 2011;88:767–77. doi: 10.1016/j.ajhg.2011.05.007. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
