

Analyzing "failure to rescue": is this an opportunity for outcome improvement in cardiac surgery?
- PMID: 23642682
- PMCID: PMC4398337
- DOI: 10.1016/j.athoracsur.2013.03.027
Analyzing "failure to rescue": is this an opportunity for outcome improvement in cardiac surgery?
Abstract
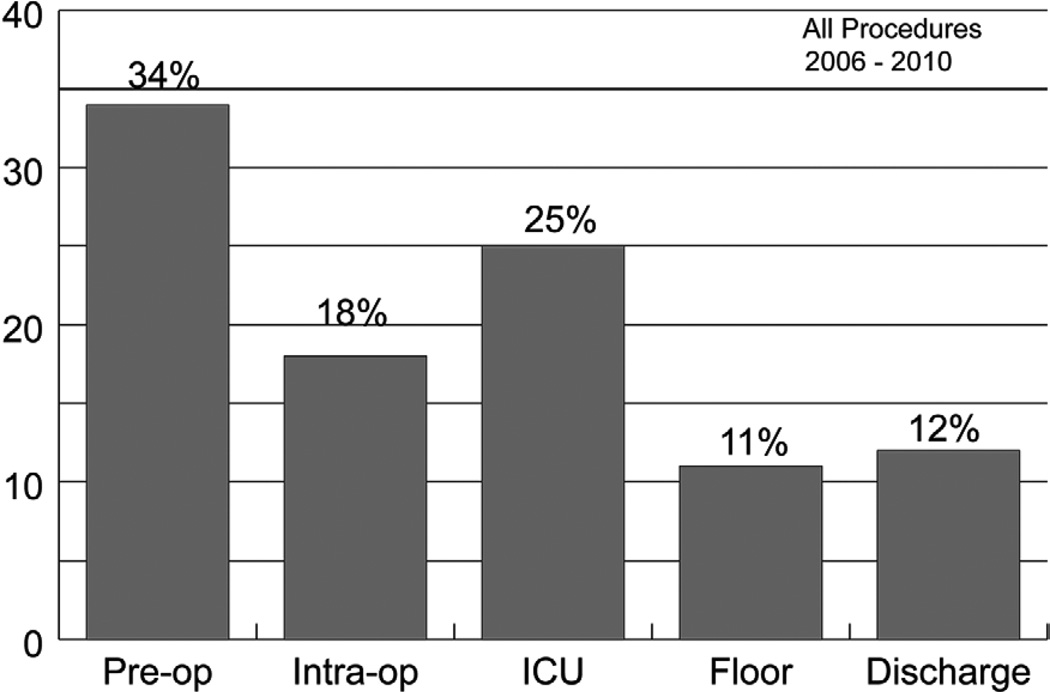
Background: In the setting of a statewide quality collaborative approach to the review of cardiac surgical mortalities in intensive care units (ICUs), variations in complication-related outcomes became apparent. Utilizing "failure to rescue" methodology (FTR; the probability of death after a complication), we compared FTR rates after adult cardiac surgery in low, medium, and high mortality centers from a voluntary, 33-center quality collaborative.
Methods: We identified 45,904 patients with a Society of Thoracic Surgeons predicted risk of mortality who underwent cardiac surgery between 2006 and 2010. The 33 centers were ranked according to observed-to-expected ratios for mortality and were categorized into 3 equal groups. We then compared rates of complications and FTR.
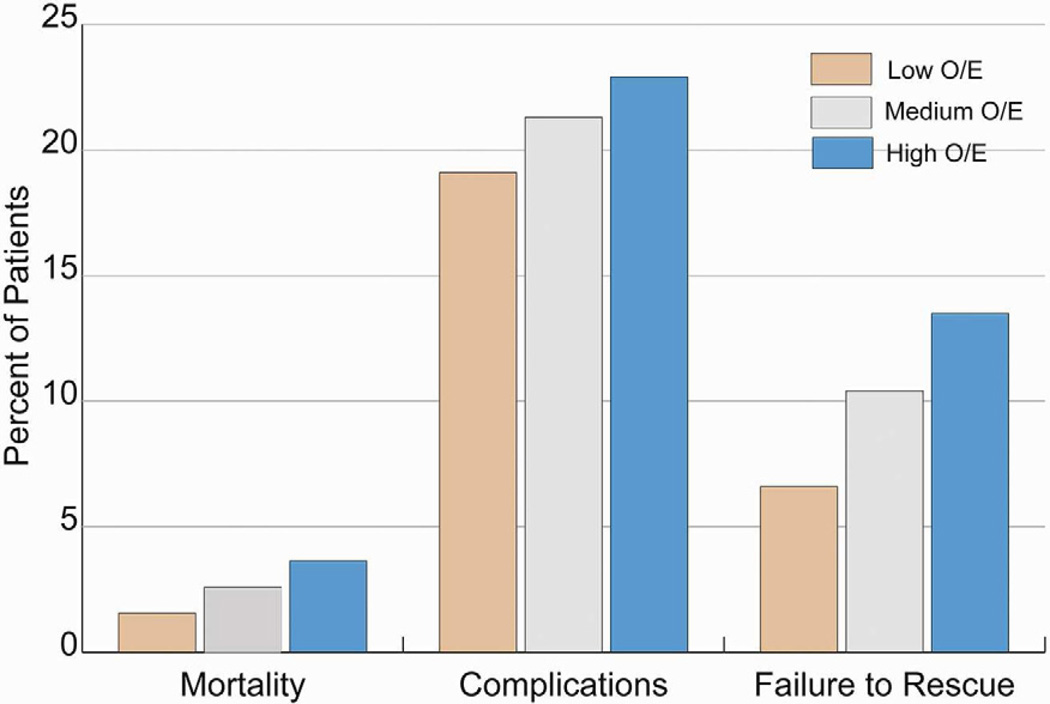
Results: Overall unadjusted mortality was 2.6%, ranging from 1.5% in the low-mortality group to 3.6% in the high group. The rate of 17 complications ranged from 19.1% in the low group to 22.9% in the high group while FTR rates were 6.6% in the low group, 10.4% in the medium group, and 13.5% in the high group (p < 0.001). The FTR rate was significantly better in the low mortality group for the majority of complications (11 of 17) with the most significant findings for cardiac arrest, dialysis, prolonged ventilation, and pneumonia.
Conclusions: Low mortality hospitals have superior ability to rescue patients from complications after cardiac surgery procedures. Outcomes review incorporating a collaborative multi-hospital approach can provide an ideal opportunity to review processes that anticipate and manage complications in the ICU and help recognize and share "differentiators" in care.
Copyright © 2013 The Society of Thoracic Surgeons. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Prager RL, Armenti FR, Bassett JS, et al. Cardiac surgeons and the quality movement: the Michigan experience. Semin Thorac Cardiovasc Surg. 2009;21:20–27. - PubMed
-
- Shannon FL, Fazzalari FL, Theurer PF, et al. A method to evaluate cardiac surgery mortality: phase of care mortality analysis. Ann Thorac Surg. 2012;93:36–43. - PubMed
-
- Ghaferi AA, Birkmeyer JD, Dimick JB. Complications, failure to rescue, and mortality with major inpatient surgery in Medicare patients. Ann Surg. 2009;250:1029–1034. - PubMed
-
- Silber JH, Williams SV, Krakauer H, Schwartz JS. Hospital and patient characteristics associated with death after surgery. A study of adverse occurrence and failure to rescue. Med Care. 1992;30:615–629. - PubMed
-
- Ghaferi AA, Birkmeyer JD, Dimick JB. Variation in hospital mortality associated with inpatient surgery. N Engl J Med. 2009;361:1368–1375. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
