

Feasibility of coronary artery wall thickening assessment in asymptomatic coronary artery disease using phase-sensitive dual-inversion recovery MRI at 3T
- PMID: 23642801
- PMCID: PMC3729736
- DOI: 10.1016/j.mri.2013.03.011
Feasibility of coronary artery wall thickening assessment in asymptomatic coronary artery disease using phase-sensitive dual-inversion recovery MRI at 3T
Abstract
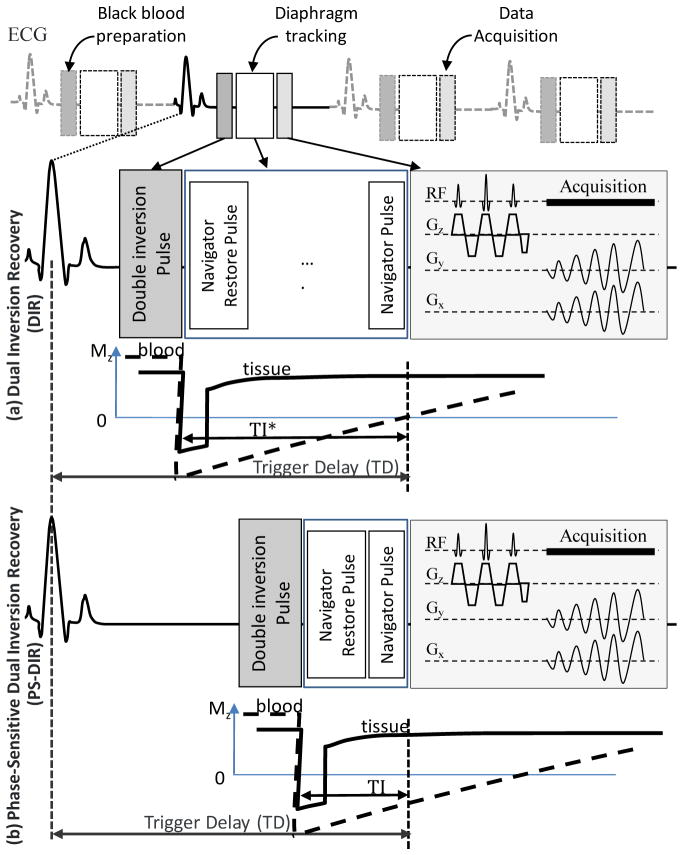
Objectives: The purpose of this study was to (a) investigate the image quality of phase-sensitive dual-inversion recovery (PS-DIR) coronary wall imaging in healthy subjects and in subjects with known coronary artery disease (CAD) and to (b) investigate the utilization of PS-DIR at 3T in the assessment of coronary artery thickening in subjects with asymptomatic but variable degrees of CAD.
Materials and methods: A total of 37 subjects participated in this institutional review board-approved and HIPAA-compliant study. These included 21 subjects with known CAD as identified on multidetector computed tomography angiography (MDCT). Sixteen healthy subjects without known history of CAD were included. All subjects were scanned using free-breathing PS-DIR magnetic resonance imaging (MRI) for the assessment of coronary wall thickness at 3T. Lumen-tissue contrast-to-noise ratio (CNR), signal-to-noise ratio (SNR) and quantitative vessel parameters including lumen area and wall thickness were measured. Statistical analyses were performed.
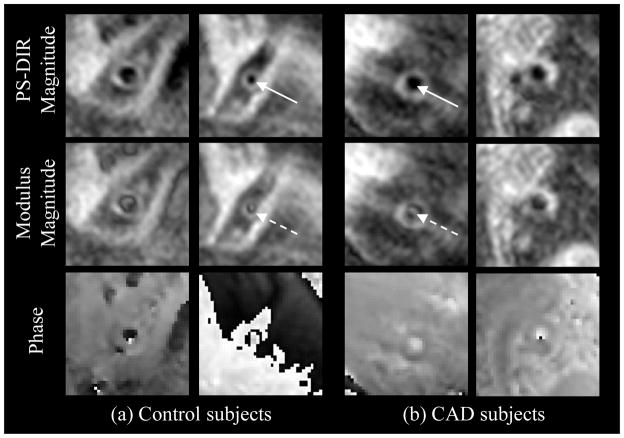
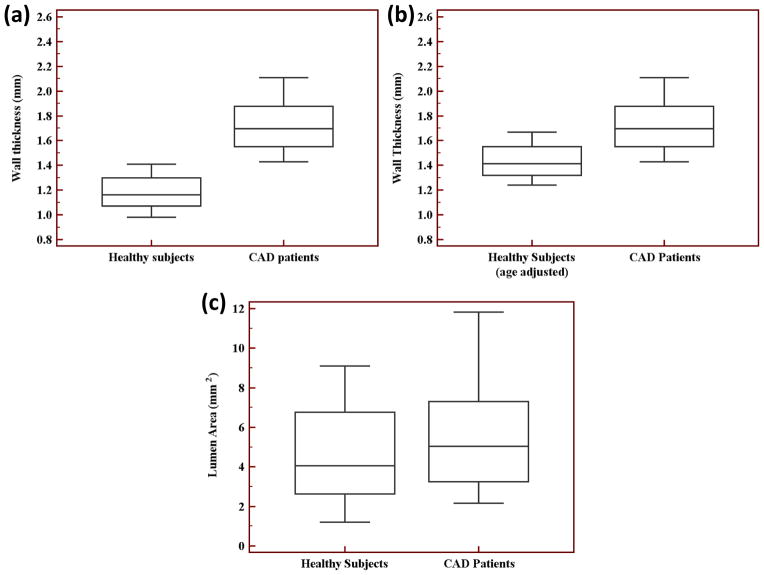
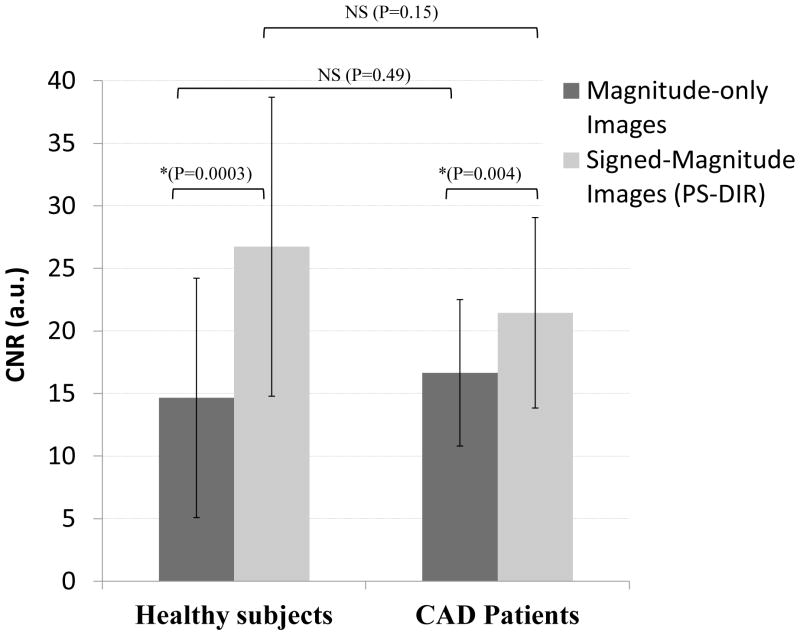
Results: PS-DIR was successfully completed in 76% of patients and in 88% of the healthy subjects. Phase-sensitive signed-magnitude reconstruction, compared to modulus-magnitude images, significantly improved lumen-tissue CNR in healthy subjects (26.73±11.95 vs. 14.65±9.57, P<.001) and in patients (21.45±7.61 vs. 16.65±5.85, P<.001). There was no difference in image CNR and SNR between groups. In arterial segments free of plaques, coronary wall was thicker in patients in comparison to healthy subjects (1.74±0.27 mm vs. 1.17±0.14 mm, P<.001), without a change in lumen area (4.51±2.42 mm2 vs. 5.71±3.11mm2, P=.25).
Conclusions: This is the first study to demonstrate the feasibility of successfully obtaining vessel wall images at 3T using PS-DIR in asymptomatic patients with known variable degrees of CAD as detected by MDCT. This was achieved with a fixed subject-invariant planning of blood signal nulling. With that limitation alleviated, PS-DIR coronary wall MRI is capable of detecting arterial thickening and positive arterial remodeling at 3T in asymptomatic CAD.
Keywords: 3T; Atherosclerosis; Black blood MRI; Coronary artery imaging; Dual-inversion recovery; Phase sensitive; Vessel wall.
Published by Elsevier Inc.
Figures
References
-
- Kim WY, Danias PG, Stuber M, et al. Coronary magnetic resonance angiography for the detection of coronary stenoses. N Engl J Med. 2001;345(26):1863–9. - PubMed
-
- Sakuma H, Ichikawa Y, Suzawa N, et al. Assessment of coronary arteries with total study time of less than 30 minutes by using whole-heart coronary MR angiography. Radiology. 2005;237(1):316–21. - PubMed
-
- Sommer T, Hackenbroch M, Hofer U, et al. Coronary MR angiography at 3.0 T versus that at 1.5 T: initial results in patients suspected of having coronary artery disease. Radiology. 2005;234(3):718–25. - PubMed
-
- Sakuma H, Ichikawa Y, Chino S, Hirano T, Makino K, Takeda K. Detection of coronary artery stenosis with whole-heart coronary magnetic resonance angiography. J Am Coll Cardiol. 2006;48(10):1946–50. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
